


Introduction
Health statistics for children 5 years of age and under are frequently used as a barometer of a population's health because they provide valuable information regarding the status of society's most vulnerable in terms of a healthy start in life for optimal growth and development, and longevity. Population health is influenced by a broad range of factors that go beyond traditional health and health care measures, and include a 'range of personal, social, and economic factors'1,2. Further, for Indigenous peoples, health determinants include a dimension related to 'indigeneity' where disassociation from land and culture are now recognized for their contribution to health disparities3. For children's health, poverty is considered a leading threat4 and, because young children spend the majority of their time at home, the home environment is a central determinant of health. Further, there is a recognized interplay of factors ranging from the family and home environment to genetic factors and the broader society, all of which impact on children's health and development5.
In Canada, unemployment and poverty rates are twice as high among Indigenous peoples than non-Indigenous peoples6-7, and Inuit, who reside in 52 remote communities without road access, known collectively as Inuit Nunaat, face even greater challenges due to high unemployment rates and low incomes6, coupled with a high cost of living8-9 and poor access to health care10. Further, most health indicators identify large disparities in morbidity and longevity among Indigenous peoples relative to the general Canadian population, with a gap in life expectancy of 5.5 years for females and 8.1 years for males in 200011. However, for Inuit, the average life expectancy is estimated to be 15 years shorter than that of the Canadian population12. Further, infant mortality rates among Inuit, while decreasing over time, remains four times higher than among the general Canadian population12.
Given the health disparities noted between Inuit and non-Inuit and the lack of information on population health indicators in early childhood, an Inuit Child Health Survey was conducted in Nunavut Territory of Canada as part of a larger International Polar Year Inuit Health Survey (www.inuithealthsurvey.ca). To date the study has reported on a number of health determinants, including a high prevalence of child food insecurity (56%)13, a high degree of adiposity based on US14 and international growth standards13, a high intake of nutrient-poor but energy-dense beverages and food items15, and a high prevalence of reported extracted, filled or decayed deciduous teeth16.
The present report focuses on additional population-based health indicators covering three domains: (i) indigeneity; (ii) physical and socioeconomic environment; and (iii) health behaviours and health histories.
Methods
Study population
A cross-sectional health survey was conducted in the late summer and fall of 2007 and 2008 in 16 selected communities of the 25 communities of Nunavut, representing all 3 regions of the Canadian territory. The communities included in the survey were: Arviat, Baker Lake, Cambridge Bay, Chesterfield Inlet, Clyde River, Coral Harbour, Igloolik, Iqaluit, Kimmirut, Kugaaruk, Kugluktuk, Pangnirtung, Pond Inlet, Rankin Inlet, Sanikiluaq, and Whale Cove (Fig1). Selection of communities was based on achieving representation in terms of community size (small, medium, large), latitude, and region and the logistical feasibility of scheduled airline routes. The combined total population of Inuit 3-5 year olds in the 16 communities during the 2 years of data collection was 1487 and this was based on health centres' records of age-appropriate children. These 16 communities, in turn, represent 76.4% of 3-5 year old Inuit children in Nunavut (Statistics Canada; unpubl. data, 2006). The latitude of the communities ranged from 56o 32'N to 72o 40'N. Certain communities were not included due to their very small number of age-appropriate children relative to costs, and the logistic constraints of restricted flight schedules.
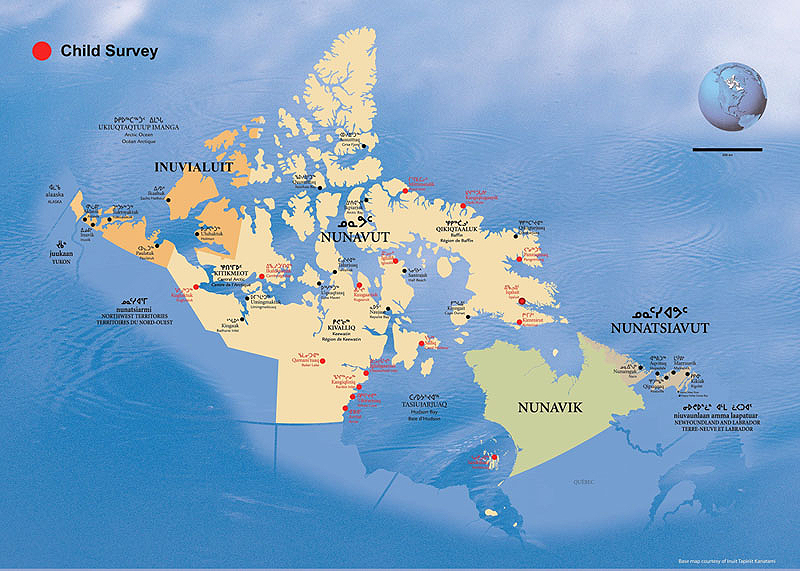
Figure 1: Participating communities (in red) of the Nunavut Inuit Child Health Survey, 2007-2008.
All Inuit children aged 3-5 years residing in each of the selected communities were eligible to participate and were randomly recruited through: (i) randomized community health centres' lists of age-appropriate children; and (ii) a list of randomly selected households with 3-5 year olds who participated in the International Polar Year Adult Inuit Health Survey for Nunavut. In the event of more than 2 age-appropriate children per household, the child with the birthday closest to the time of the clinic was selected. A total of 537 households with 3-5 year olds were successfully contacted, of whom 75 refused participation on initial contact, and an additional 74 cancelled or failed to attend their clinic visit, thereby providing a 72.3% participation rate with 388 participants. The 388 children represent 26% of all Inuit 3-5 year olds in the 16 communities, based on the health centres' records of age-appropriate children. A total of 12 to 35 children participated per community.
Ethics and participatory processes
The study was developed in a participatory process17 with the Nunavut Inuit Health Survey Steering Committee Qanuippitali? What about us, how are we?. The committee includes representation from the Nunavut Association of Municipalities, the Nunavut Tunngavik Incorporated, the Government of Nunavut Department of Health and Social Services, University of Toronto, and the Centre for Indigenous Peoples' Nutrition and Environment (CINE), McGill University. The steering committee was active in determining the content of the child health survey. A Scientific Research License was obtained from the Nunavummi Qaujisaqtulirijikkut (the Nunavut Research Institute). The McGill Faculty of Medicine Institutional Review Board issued a certificate of ethical acceptability. Written and signed informed consent forms were administered following viewing of an informational DVD available in Inuktitut, Inuinnaqtun and English.
For both years of data collection, the research team included bilingual Inuk interviewer/s, two CINE research assistants, and a nurse. Local assistants were hired as needed to facilitate the recruitment of study participants. The nurse asked all the health related questions and performed all clinical measurements. The research team was trained in administering the questionnaires, and quality control of questionnaires was conducted in the field by the CINE staff.
Face-to-face interviews with parents and primary caregivers covered household characteristics, health histories, and histories of pregnancy and early infant feeding.
Indigeneity
The domain of indigeneity refers to items of interest to Inuit partners and involve indicators of culture and acculturation, social cohesion and social safety nets, as specified among the determinants of Inuit health during a workshop held in Nunavut in 2005 and reported by the Aboriginal Peoples' Survey18. Traditional food, also known as 'country food', is central to Inuit identity and cultural cohesion; hunting and harvesting of food, food sharing networks, and community feasts provide social support, cohesion and cultural identity. Thus, the household questionnaire included items such as whether there was an active hunter in the home, whether the household distributed country food to others in the community, food preference, means of obtaining country food, whether parents worried about contaminants in their country food, and if they preferred eating more country food than they could obtain. The primary language spoken by the child, detail of who provided most care for the child, and daycare attendance were also assessed.
Physical and social-economic environment
The home questionnaire and household composition form included items on the number, ages and gender of all household members; the type of housing (public or private/job-related housing); whether the home was in need of major repairs; the number of smokers in the home and restrictions against smoking in the home; the number of bedrooms; whether the home had taken in homeless visitors in the past year; and household expenses, and any income support by a household member. For household crowding, Statistics Canada's definition of more than one person per room was used, where rooms included bedrooms, kitchen and living room6.
Health behaviours and health
Fetal and early infant exposure information included the biological mother's intake of prenatal vitamins, her alcohol consumption and smoking during pregnancy, and the history of breastfeeding.
The parent or primary caregivers' subjective assessment of the child's health (excellent, very good, good, fair, and poor) was assessed. The child's health history included questions on allergy, asthma, injury, ear infection/earaches, respiratory illness, and hospitalizations.
Database management and statistical analyses
All data were entered into Microsoft Access Database designed for the Inuit Child Health Survey using MS Access 2003; data were subsequently checked by a quality control team for any data entry errors. There was a low prevalence of missing data for questionnaire items; however, the top three variables for missing data were household crowding (missing for 5.7%, n = 22); ever hospitalized (missing for 6.4%, n = 25); and weekly market food costs (missing for 12.6%, n = 49).
Weighted prevalence estimates and 95% confidence intervals (CI) of survey responses were calculated using SAS v9.2 (SAS Institute Inc.; Cary, NC; USA). The denominator of age-appropriate Inuit children was obtained from community health centers' records.
Results
Demographic characteristics
Of the 388 participating children, 184 were boys and 204 were girls. The majority of primary caregivers interviewed were either biological (68.4%) or adoptive (21.6%) parents, the remaining 10% were either a grandparent, aunt or uncle or other primary caregiver. The majority of respondents were female (87.4%). The mean age of participating children was 4.4 years (SD=0.9).
Indigeneity
The majority of children had daily contact with extended family (69.7%), parents provided the most care for the child in the majority of cases (84%), and the majority of children usually stayed at home during the day (64.5%) with the remainder in homecare or daycare (Table 1). The primary language spoken by the children was Inuktitut (47.9%) or English (43.6%), with 7.7% speaking both English and Inuktitut. In Inuktitut speaking Baffin and Kivalliq Regions, 65.2% (95% CI: 61.2-69.1) of children spoke Inuktitut. Only one adult reported speaking Inuinnaqtun with preschoolers as their primary language (the Inuinnaqtun language is found in central and western areas of the Kitikmeot region).
Table 1: Weighted characteristics of indigeneity and physical and socio-economic environment: Nunavut Inuit Child Health Survey, 2007-2008
Questions concerning country food indicated that country food utilization is prevalent with 70.9% of preschoolers residing in a home with an active hunter, 81.2% residing in a home that distributed country food to other members of the community, and 75.6% receiving traditional food from family and friends in the past year. The majority of respondents indicated that they preferred a mixture of store-bought and traditional foods (82%) and that they preferred eating more country food than they can get (82.7%), while almost 33% worried about contaminants in country food.
Physical and socioeconomic environment
The weighted average number of individuals living in a household was 5.9, with 53.9% of children residing in a crowded dwelling. The prevalence of single-adult headed households was 10.3% (95% CI: 7.4-13.2%). The majority of children resided in public housing (69.7%), and in a home where at least one household member received income support (42.7%) (Table 1). Thirty-seven percent of preschoolers resided in a home in need of major repairs, and almost 12% of children lived in homes where an average of 2 homeless visitors had stayed in the past year.
On average, families reported that they spent CND$428 a week on food and $894 on other household expenses, including rent, electricity, heating fuel, gas, water, sewage and garbage removal, skidoo parts and oil, bullets, and other essential materials.
There was an average of 2 cigarette smokers per home but it was commonly reported (83.1%) that smoking was entirely forbidden in the home (Table 1).
Health behaviours and health histories
Any cigarette smoking during pregnancy was very common (82.5%) with the average number of cigarettes smoked being 9 cigarettes/day (95% CI: 8.4-10.0). Alcohol consumption during pregnancy was reported for 24.2%, with 5 or more drinks on any one occasion during pregnancy reported by 8.6% of biological mothers. The weighted prevalence of children who were ever fed breast milk was 67.6%, but in analyses excluding children with an adoptive parent, the prevalence of children ever breastfed was 80.6% (95% CI: 75.6-85.5). The mean number of months a child was fed any breast milk was 17.4 months (95% CI: 15.3-19.7). Approximately 30% of the biological mothers reported not ever taking a prenatal vitamin or multivitamin during the pregnancy; whereas 38% reported taking a vitamin more than 30 times (Table 2). Among those taking any vitamins or supplements, only 26% reported taking any vitamin D during pregnancy, and 83.1% reported taking any iron or folate.
Table 2: Weighted Prevalence Health Behaviour and Health Indicators: Nunavut Inuit Child Health Survey, 2007-2008
The weighted prevalence of caregivers' assessment of child health was excellent, very good, good, fair, and poor for 22.8%, 31.6%, 37.3%, 7.7%, and 0.5%, respectively. Respondents reported past-year ear infections or earache for 36.4% of children with 12.3% suffering from 6 or more episodes in the past year. A high prevalence (41.6%) of children were reported to ever have been hospitalized (excluding deliveries) and, within the past year, 40.7% of the children had had to be taken to the health centre or hospital for a respiratory problem. In contrast, allergies, asthma, a chronic disability or illness, and past-year injury were not as commonly reported (4.9%, 4.0%, 4.9%, and 9.0%, respectively). The majority of injuries reported were minor scratches and bruises. Almost 23% of children currently took a vitamin or supplement, with vitamin C and multivitamins being the most frequently taken.
Discussion
Indigeneity
Positive elements of the survey findings included the high prevalence of children who had with contact with extended family, and who were living in homes where country food is utilized and shared, and where Inuktitut is spoken. All of these factors indicated that Inuit children are learning Inuit ways and that social support networks are in operation. Social safety nets and indicators of acculturation are among the top 11 determinants of Inuit health according to participants in an Inuit Social Determinants of Health workshop held in Nunavut in 2005 and reported by Aboriginal Peoples' Survey (APS)18. In the 2006 APS, 68% of Inuit Nunaat reported participating in the hunting and harvesting of country food in the previous year18, a similar prevalence to that found in the current survey where 70% of preschoolers were living in a home with an active hunter. Further, 8 in 10 Inuit reported sharing country food with others in the previous year in the 2006 APS18, which is comparable to 81% of preschoolers' homes reporting sharing country food with others in the present study.
Physical and social-economic environment: household characteristics
An overarching public health problem area identified by the present study involves the high degree of household crowding, homes in need of major repairs, public housing, and income support, all of which indicate chronic economic and social disadvantage with consequences for population health. According to a 2006 Census, 38% of Inuit living in Inuit Nunaat lived in crowded homes compared with 3% of the Canadian population6. For Inuit children, 43% lived in crowded homes, approximately 6 times greater than for non-Aboriginal children (7%) in Canada19. Using the same definition of household crowding, the present study identified a higher prevalence of household crowding for the preschoolers in the 16 Nunavut communities (54%). In an assessment of Inuit community wellbeing, Indian and Northern Affairs Canada developed an index based on education, labour force activity, income and housing, and found substantial disparities within Inuit communities and between Inuit and non-Inuit communities in Canada, with household crowding and condition of dwelling accounting for half the gap in the community wellbeing score20. In Greenland, family size was reported as 3.1 persons in villages and 2.5 persons in towns21,22. In those studies, 76% of all children lived in homes with 2 adults and 24% lived in a single-parent household in 200221,22; however, another Greenland study reported that 14.9% of children lived in a single-parent household5. In contrast, Nunavut homes consisted of extended families with few households having only one adult in the home (10.3%).
While the prevalence of homeless visitors was not excessive, it would exacerbate the already high prevalence of crowding observed in Nunavut. As young children spend most of their time in the home, household crowding is of particular concern for child health. Household crowding can lead to a host of public health problems23, including but not limited to, psychosocial stressors and violence24-25 and a greater propensity for illnesses, particularly those related to infections, such as meningococcal disease, respiratory syncytial virus infection, and tuberculousis26-31. Further, in a longitudinal study of children residing in Québec, Canada, chronic poverty was identified as a risk factor for children's development of health problems (based on a cumulative health problem index score) and for the number of asthma attacks, whereas intermittent poverty was related to maternal perceptions that their child was in less than very good health32.
The weekly food costs in the present study was three-fold higher than that reported for other Canadian households33, but differences in household size and composition between Inuit and other Canadian households make direct comparisons difficult. In general, food costs for a standard food basket for a family of 4 individuals is twice as high in remote northern communities than in southern Canadian communities8.
Health behaviours and health histories
A positive finding relates to breastfeeding. While only 67.6% of children had received any breast milk, when analyses excluded children with an adoptive parent, the prevalence of any breastfeeding and the duration of breastfeeding were fairly high. In the 2001 APS, Inuit children were reported to be less likely than all children in Canada to be breastfed, possibly attributable to differences in adoption rates. However, when Inuit children were breastfed it was for a longer duration, with the proportion of children breastfed for more than 6 months in Nunavut, Nunavik, and Labrador, being higher than the national average obtained from the National Longitudinal Survey of Children and Youth (NLSCY) Cycle 4 (2000/2001)34. In the US, Alaska (AK) has one of the highest breastfeeding initiation rates for the nation, with 91% of Alaskan mothers delivering a live born infant in 2005 reporting initiation of breastfeeding; further, no disparities in breastfeeding rates were noted between Alaska Native or non-Natives35. However, in AK, only 58% of women were breastfeeding at 16 weeks postpartum35.
Other positive elements of the current study were the relatively low prevalence of allergies (4.9%), asthma (4%), chronic disability or illness (3.9%), and past-year injuries of which the majority were minor scratches and bruises. In the 2006 APS, a higher prevalence of allergies (10%) and asthma (7%) was noted for Inuit children aged 6-14 years, while the most widely diagnosed chronic health condition for that age group was ear infections (15%)18. In the current survey of preschoolers, 36% had an ear infection/earache requiring medical attention and 86% had a positive history for having ever received treatment for an ear infection/earache. Also, the prevalence of respiratory illness was high among preschoolers; however, this was not surprising given that Inuit children have been noted to have very high rates of hospitalizations for lower respiratory tract infections26-27. Household crowding, reduced ventilation in crowded households, not being breastfed, and maternal smoking during pregnancy are among the risk factors that have been implicated for lower respiratory tract infections in various studies26-29.
While the prevalence of smoking remains high in Nunavut with 64% of those 15 years of age and older reporting daily smoking18, the high prevalence of restrictions against smoking in the home is another positive finding and indicates that public health messages designed to reduce passive smoking have had an impact on behaviours in Nunavut. However, as fetal exposure to tobacco smoke poses risk to offspring, the high percentage of mothers reporting any smoking during pregnancy in the present study is of public health concern. It should be notes, however, that daily smoking was not included in the questionnaire items; therefore, the percent reporting any smoking during pregnancy (82.5%) may slightly over-estimate the extent of daily smoking during pregnancy in Nunavut, where occasional smoking is reported18. However, the smoking prevalence observed in the present study is comparable with 2 unpublished surveys which found that 80% of pregnant mothers smoke in Nunavut (Osborne G, Deputy Chief Medical Office of Health; pers. comm., 30 October 2009). Among Greenlandic children, 57.5% had in-utero exposure to tobacco smoke5. In contrast, in AK 12% of non-Native and 27.7% of Native women smoked during the last 3 months of pregnancy in 200535.
Because children of smokers are more likely to initiate smoking36, further public health action is needed to reduce tobacco exposure in Nunavut. Another problem area identified in the present study involves prenatal alcohol exposure, indicating ongoing need for interventions to ensure an optimal start to life. In Alaska, any alcohol use during the last 3 months of pregnancy was reported for 5% of non-Native and 3.7% of Native women, and the prevalence of binge drinking was considerably less (under 1%)35 than was reported in the present study.
Only 38% of mothers reported taking a vitamin more than 30 times during pregnancy, whereas Health Canada's Food Guide recommends all pregnant women should routinely take a multivitamin containing folic acid and iron37.
The parental assessment of child's health status as excellent or very good for 54% of the preschoolers was comparable with the 50% of Inuit adults self-reporting excellent or very good health in the 2006 APS18, but lower than that was reported for Inuit children up to 14 years of age38.
Strengths and limitations
A strength of the current study is that it provides the first comprehensive look at population health indicators covering indigeneity, physical and socioeconomic environment, and health behaviours and health histories among Inuit preschoolers in Canada. The survey results are likely to be generalizable as the present study identified a similar prevalence of selected indicators to other studies, particularly involving the number of individuals living per household, the percent participating in country food acquisition and sharing networks, and in the relatively long duration of any breastfeeding6,28,34. Further, estimates of household crowding were comparable but slightly higher than that identified for Inuit households with children 15 years of age and under19. In general, the findings are comparable with the prevailing literature and provide insight into the social, economic, and physical living conditions and health status of Inuit preschoolers.
A limitation of the current survey is that it could not address all pertinent health indicators for preschoolers. Additional data such as those from healthcare services are needed to provide a more holistic assessment of preschool health status. The Government of Nunavut, Department of Health and Social Services is developing a perinatal outcome and child health surveillance system for Nunavut (from pregnancy to 4 years of age) that will provide opportunities to evaluate the population over time, to track trends, and to provide feedback on the efficacy of public health interventions. Developing maternal child health surveillance throughout Canada and in the larger Circumpolar North, and building compatibility with the existing systems in place in the US35 and Greenland5,22 will provide a basis for developing public health interventions to reduce health disparities.
Conclusion
While the Nunavut Inuit Child Health Survey identified many positive findings, the survey also identified socioeconomic hardships which, over the long-term, can have a highly a influential impact on child health and development. Adequate housing and sufficient means for sustaining a family represent the foundation for a population's good health. The findings of the present study, together with other findings emerging from the analyses of the preschool survey, suggest the need for interventions. The high prevalence of restrictions against smoking in homes suggests that public health messages have had an impact and that future efforts could continue to change health behaviours in a meaningful way. Apart from improving health behaviours, the data also suggest the need for relevant public policy and action at the community, territorial and federal level to help improve living conditions and alleviate poverty for families with young children.
As part of the current survey activities, a plain language non-technical report was sent to all communities and community health and wellness committees. Further, a plain language results DVD, which also provided public health advice in English and Inuktitut, has been produced and sent to all Nunavut communities and participating households. Knowledge translation of research findings is one means of positively influencing population health in remote communities of the Artic.
Acknowledgements
The authors thank the Nunavut Inuit Health Survey Steering Committee for their ongoing guidance; the CINE staff, particularly Dr Nelofar Sheikh for database management, and Zhirong Cao for statistical analyses support; the members of the field research child health survey team, and participating communities and families.
References
1. WHO. Health promotion glossary. (Online) 1998. Available: http://whqlibdoc.who.int/hq/1998/WHO_HPR_HEP_98.1.pdf (Accessed 1 March 2010).
2. Glouberman S, Millar J. Evolution of the determinants of health, health policy, and health information systems in Canada. Americal Journal of Public Health 2003; 93(3): 388-392.
3. King M, Smith A, Gracey M. Indigenous health part 2: the underlying causes of the health gap. Lancet 2009; 374(9683): 76-78.
4. World Health Organization Regional Office for Europe. Public health action for healthier children and populations. The European Health Report 2005. Copenhagen: World Health Organization, 2005.
5. Niclasen B, Köhler L. National indicators of child health and well-being in Greenland. Scandinavian Journal of Public Health 2009; 37: 347-356.
6. Statistics Canada. Aboriginal Peoples in Canada in 2006: Inuit, Métis, and First Nations, 2006 Census: findings. Ottawa, ON: Statistics Canada, 2006. Available: http://www12.statcan.gc.ca/census-recensement/2006/as-sa/97-558/index-eng.cfm (Accessed 13 April 2010).
7. Anderson J. Aboriginal children in poverty in urban communities. Social exclusion and the growing racialization of poverty in Canada. Ottawa, ON: Canadian Council on Social Development, 2003. Available: http://www.ccsd.ca/pr/2003/aboriginal.htm (Accessed 20 August 2009).
8. Indian and Northern Affairs Canada. Revised Northern Food Basket. Ottawa, ON: Indian and Northern Affairs Canada, 2008. Available: http://www.ainc-inac.gc.ca/nth/fon/fc/hpsr-eng.asp (Accessed 13 April 2009).
9. Bernard N. Nunavik Comparative Price Index, 2006. Québec, QC: Chaire Condition Autochtone, Université Laval, 2006. Available: http://www.chaireconditionautochtone.fss.ulaval.ca/en/PDF/Nunavik%20Comparative%20Price%20Index%202006.pdf (Accessed 13 April 2010).
10. Health Canada. Health Care System. Part I. Equity in access to health care. Access to health services for underserved populations in Canada. Section 4: Underserved populations in Canada. (Online) 2004. Available: http://www.hc-sc.gc.ca/hcs-sss/pubs/acces/2001-certain-equit-acces/part1-doc1-sec4-eng.php (Accessed 1 March 2010).
11. Health Canada. First Nations, Inuit and Aboriginal health. Life expectancy at birth for overall population. (Online) 2007. Available: http://www.hc-sc.gc.ca/fniah-spnia/diseases-maladies/2005-01_health-sante_indicat-eng.php#life_expect (Accessed 27 October 2009).
12. Wilkins R, Uppal S, Finès P, Senécal S, Guimond E, Dion R. Life expectancy in the Inuit-inhabited areas of Canada, 1989-2003. Health Reports 2008; 19(1). Available: http://www.statcan.gc.ca/pub/82-003-x/82-003-x2008001-eng.htm (Accessed 27 October 2009).
13. Egeland GM, Pacey A, Cao Z, Sobol I. Food Insecurity Among Inuit Prescholers: Nunavut Inuit Child Health Survey, 2007-2008. Canada Medical Association Journal 2010; 182(3): 243-248.
14. Galloway T, Young T.K., Egeland GM. Emerging obesity among preschool-aged Canadian Inuit Children: The Nunavut Inuit Child Health Survey, 2007-2008. International Journal of Circumpolar Health 2010; 69(2): (in press).
15. Johnson-Down L, Egeland GM. Adequate nutrient intake is associated with traditional food consumption in Nunavut Inuit children 3-5 years old. Journal of Nutrition 2010; (in press).
16. Pacey A, Nancarrow T, Egeland GM. Prevalence and risk factors for parental-reported oral health of Inuit preschoolers: Nunavut Inuit Child Health Survey, 2007-2008. Rural and Remote Health. 10: 1368. (Online) 2010. Available: www.rrh.org.au (Accessed 18 June 2010).
17. WHO and CINE. Indigenous peoples and participatory health research. Geneva: World Health Organization and Centre for Indigenous Peoples' Nutrition and Environment, 2003.
18. Tait H. Aboriginal Peoples Survey, 2006: Inuit health and social conditions. Ottawa, ON: Statistics Canada, 2008. (Online) 2006. Available: http://dsp-psd.pwgsc.gc.ca/collection_2008/statcan/89-637-X/89-637-x2008001-eng.pdf (Accessed 13 April 2010).
19. Statistics Canada. 2006 Census. Inuit children. Ottawa: Ontario, Statistics Canada, 2008. Available: http://www.fsin.com/healthandsocial/childportal/images/89-634-XIE2008004.pdf (Accessed 27 October 2009).
20. Inuit Relations Secretariat. Measuring Inuit Well Being. Indian and Northern Affairs Canada, Ottawa: ON, 2006. Available: http://www.ainc-inac.gc.ca/ai/rs/pubs/re/miwb/miwb-eng.asp (Accessed 27 October 2009).
21. Meeqqat Inuusuttullu Pillugit Illisimasaqarfik [Documentation Centre on Children and Youth]. Familiers levevilkar 2004. [Statistics on children and youth in Greenland]. Nuuk: Greenland Homerule; 2004. In: Niclasen BVL, Bjerregaard P. Child health in Greenland. Scandinavian Journal of Public Health 2007; 35: 313-322.
22. Niclasen BVL, Bjerregaard P. Child health in Greenland. Scandinavian Journal of Public Health 2007; 35: 313-322.
23. Public Health Agency of Canada. The Chief Public Health Officer's Report on the state of public health in Canada 2008. (Online) 2008. Available: http://198.103.98.77/publicat/2008/cphorsphc-respcacsp/index-eng.php (Accessed 13 April 2010).
24. Fuller TD, Edwards JN, Vorakitphokatorn S, Sermsri S. Chronic stress and psychological well-being: evidence from Thailand on household crowding. Social Science and Medicine 1996; 42(2): 265-80.
25. Centerwall BS. Race, socioeconomic status, and domestic homicide. JAMA 1995; 273(22): 1755-1758.
26. Banerji A, Greenberg D, White LF, Macdonald WA, Saxton A, Thomas E et al. Risk factors and viruses associated with hospitalization due to lower respiratory tract infections in Canadian Inuit children: A case-control study. Pediatric Infectious Disease Journal 2009; 28(8): 697-701.
27. Banerji A, Bell A, Mills EL, McDonald J, Subbarao K, Stark G et al. Lower respiratory tract infections in Inuit infants on Baffin Island. Canada Medical Association Journal 2001; 164(13): 1847-1850.
28. Kovesi T, Stocco C, Fugler D, Dales R, Guay M, Miller J. Indoor air quality and the risk of lower respiratory tract infections in young Canadian Inuit children. Canada Medical Association Journal 2007; 177(2): 155-160.
29. Bulkow LR, Singleton RJ, Karron RA, Harrison LH. The Alaska RSV Study Group. Risk Factors for severe respiratory syncytial virus infection among Alaska Native children. Pediatrics 2002; 109(2): 210-216.
30. Baker MF, McNicholas A, Garrett N, Jones N, Stewart J, Koberstein V et al. Household crowding a major risk factor for epidemic meningococcal disease in Auckland children. The Pediatric Infectious Disease Journal 2000; 19(10): 983-990.
31. Baker M, Das D, Venugopal K, Howden-Chapman P. Tuberculosis associated with household crowding in a developed country. Journal of Epidemiology and Community Health 2008; 62: 715-721.
32. Séguin L, Nikiéma B, Gauvin L, Zunzunegui MV, Xu Q. Duration of poverty and child health in the Québec Longitudinal Study of Child Development: Longitudinal analyses of a birth cohort. Pediatrics 2007; 119(5): e1063-1070.
33. Statistics Canada. Survey of household spending. (Online) 2009. Available: http://www.statcan.gc.ca/pub/62-202-x/2006000/t001-eng.htm (Accessed 14 October 2009).
34. Statistics Canada. Aboriginal Peoples Survey, 2001. Ottawa, ON: Statistics Canada, 2001. Available: http://www.statcan.gc.ca/pub/89-627-x/2007003/t/4129611-eng.htm (Accessed 27 October 2009).
35. Schoellhorn KJ, Perham-Hester KA, Goldsmith YW. Alaska maternal and child health data book 2008: health status edition. Anchorage, AK: Maternal and Child Epidemiology Unit, Section of Women's, Children's and Family Health, Division of Public Health, Alaska Department of Health and Social Services, 2008.
36. Wilkinson AV, Shete S, Prokhorov AV. The moderating role of parental smoking on their children's attitudes toward smoking among a predominantly minority sample: a cross-sectional analyses. Substance Abuse and Treatment, Prevention and Policy 2008; 3: 18.
37. Health Canada. Health Canada's food guide. (Online) no date. Available: http://www.hc-sc.gc.ca/fn-an/alt_formats/hpfb-dgpsa/pdf/food-guide-aliment/print_eatwell_bienmang-eng.pdf (Accessed 28 April 2010).
38. Guèvremont A, Kohen D. Inuit children's health: a report using the 2001 Aboriginal Peoples Survey (Children and Youth Component). Ottawa, Ontario: Statistics Canada, 2001. Available: http://www.statcan.gc.ca/pub/89-627-x/89-627-x2007003-eng.htm (Accessed 3 May 2010).