

Introduction
Smoking is one of the major public health problems worldwide. It is a major risk factor for heart and lung disease and contributes to the pathogenesis of many major forms of cancer, most notably lung cancer1. Tobacco smoke increases the risk for disease not only in current smokers, but also in people exposed unwillingly2. According to projections, tobacco use was responsible for causing 6.4 million deaths worldwide in 20153. The resulting disability, due to the chronicity and severity of the tobacco-attributable disease, the increased health costs (including treatment, rehabilitation and lost work days) and most importantly the early loss of life weigh heavily upon health systems and societies4,5.
Greece ratified the WHO Framework Convention on Tobacco Control in 2005 and has taken steps to control the tobacco epidemic by banning smoking in public indoor spaces, regulating advertisement and promotion of tobacco products. However, these measures haven’t proved effective overall6. According to the recent Global Adult Tobacco Survey (GATS) Greece, the overall national prevalence of smoking is 38.2%7 and it is one of the highest rates of adult smoking in the European Union8. Exposure to secondhand smoke remains very high, particularly in indoor workplaces, restaurants, bars and coffee shops9.
Although there are many recent national studies on smoking epidemiology in Greece, very few pertain exclusively to rural populations, such as the present study. The primary goal of this study was to record the prevalence of smoking and the characteristics of smokers and, second, the factors affecting smoking status, exposure to secondhand smoke and the efficacy of anti-tobacco policies in a rural area.
Methods
A cross-sectional survey was conducted in a rural area of Thessaly, central Greece. The target population included all the permanent residents of a borough, namely non-institutionalized adult (≥18 years) men and women. The total population was 13 396 residents and was distributed in 18 villages, each with a population ranging from 103 to 2357 residents10.
Sampling frame
Participants were selected by a combination of stratified sampling with probability proportional to size, random sampling and convenience sampling. First, all the villages of the study area were grouped in five strata according to their population (0–349 residents, 350–699 residents, 700–999 residents, 1000–1999 residents, >2000 residents). Then, one village from each stratum was selected with probability proportional to size. The required sample size for each village was calculated based on the age and gender demographic characteristics of the borough according to the 2011 Population Census10.
Data collection
Data were collected using the GATS questionnaire translated in Greek by the National School of Public Health7. The use of a standardized questionnaire would allow area-specific comparisons with similar studies. Apart from demographics and smoking habit questions, the questionnaire included sections about smoking cessation, secondhand smoke exposure, and attitudes about smoking policy and knowledge about the health effects of smoking.
Sampling was conducted in early 2014 by a team of trained interviewers. Starting from the village center, a street was randomly selected and the sampling team visited all the households; one member of each household was randomly selected to participate. Neighborhood and household selection was repeated until the required sample for each participating village was achieved. Empty houses and cases of refusal to participate were indexed as ‘non-participation’ and were not included in analyses.
Smoking indexes
Smoking indexes were calculated according to the GATS manuals for data analysis and presentation11. Participants who had smoked daily or occasionally during the past 30 days before the time of the study were considered smokers. On the contrary, those who never smoked in their lives or smoked in the past, either daily or occasionally, were categorized as non-smokers. Tobacco exposure was defined as the proportion of those who reported that they were exposed to tobacco during the past 30 days before the time of the study among the population of interest. For the workplace exposure index, the population of interest was respondents working in closed indoor spaces, while only non-smokers were included for the respective indexes of public or private indoor spaces (eg restaurants, bars).
Statistical analysis
Statistical analysis was performed with the Statistical Package for the Social Sciences v21.0 (IBM; http://www-01.ibm.com/software/analytics/spss/) using the complex samples module. Qualitative variables are presented as frequencies with weighted percentages and 95% confidence intervals (95%CIs) and quantitative variables as mean with standard deviation and range. For the univariate analysis, Pearson’s χ² test was used to probe for association of smoking and secondhand smoke exposure with demographics (factors). The factors that were found statistically significant in the univariate analysis were included in the logistic model. The odds ratio (OR) with the corresponding 95%CIs are presented. The general linear model was used to assess the between-sex differences in the age of smoking initiation and in consumption.
A result was considered significant when the p-value was less than 0.05.
Ethics approval
The protocol and conduction of the study was reviewed and approved by the Steering Committee of the postgraduate program Applied Public Health and Environmental Hygiene of the Medical Faculty of University of Thessaly, Greece (project identification code 1/2014). Initially, all participants were informed about the aim and methods of the study. Further, upon assurance that participation was voluntary and that responses would be anonymous and confidential, return of a completed questionnaire indicated informed consent.
Results
In total, 330 residents, namely 168 men and 162 women, were enrolled. Of the 439 selected households for the survey, 337 participated in the study (household response rate 76.8%) and 300 out of 337 questionnaires were completed (person response rate 97.9%). The total survey response rate was 75.2%.The mean age of the sample was 54.2±17.75 years (range 18.5–86.1 years). The detailed demographic characteristics of the sample are shown in Table 1.
Table 1: Selected demographic characteristics of the sample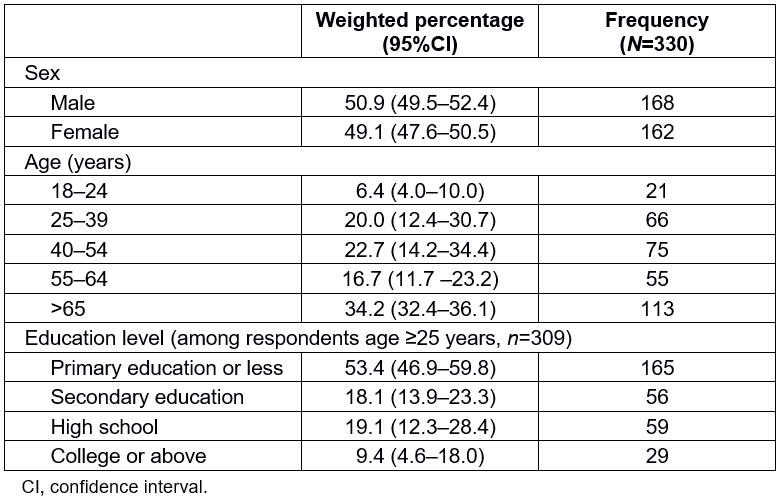
Prevalence of smoking
Almost one in three people (32.4%, 95%CI 27.5–37.8%) were current smokers. As shown in Table 2, 46.4% (95%CI 37.8–55.3%) of men and 17.9% (95%CI 12.0–25.9%) of women were smokers. Nearly all the smokers, both men and women, were daily smokers. More men than women were former smokers (36.3%, 95%CI 32.0–40.9% vs 8.0%, 95% CI 4.6–13.5%, respectively), while the opposite was noted for never smokers (17.3%, 95%CI 8.5–32.0% vs 74.1%, 95%CI 65.5–81.1%, respectively). Smoking was very common among rural residents aged 18–24 years (47.6%, 95%CI 29.2–66.7%), with the highest prevalence recorded among individuals aged 25–39 years (48.5%, 95%CI 29.9–67.5%) and the lowest at the age group of ≥65 years (16.8%, 95%CI 11.0–24.9%). Only 23.6% (95%CI 15.6–34.1%) of the participants with primary or lower education identified themselves as current smokers, while smoking was very common among secondary education graduates (46.6%, 95%CI 30.4–63.2%) and high school graduates (39%, 95%CI 29.2–49.7%) (Table 3).
The multivariate analysis showed that sex and age were significant demographic predictors of smoking in the study population (Table 4). Men were 4.33 times more likely to smoke than women (95%CI 2.69–6.97; p=0.001). A downward trend for the probability of being a smoker with increasing age was recorded.
Table 2: Prevalence of smoking among adults ≥18 years, by smoking status and sex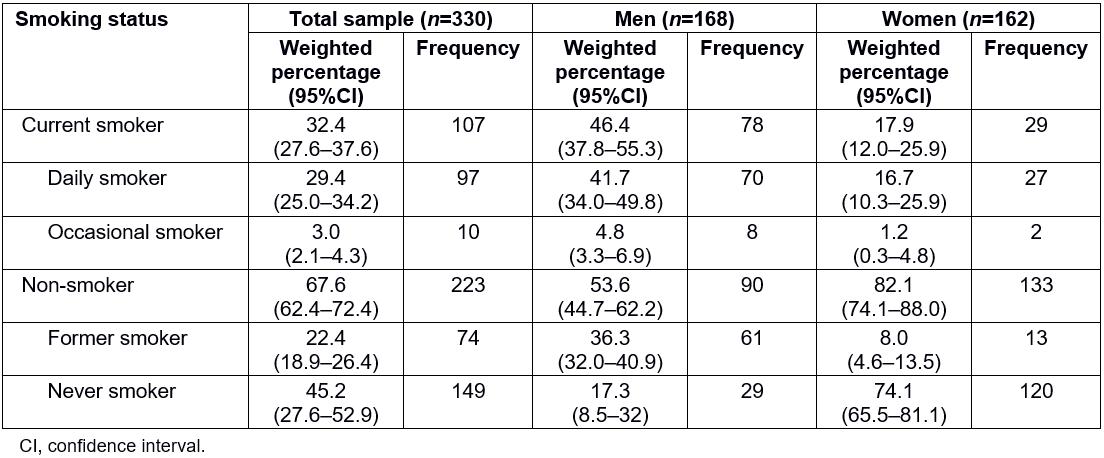
Table 3: Demographic characteristics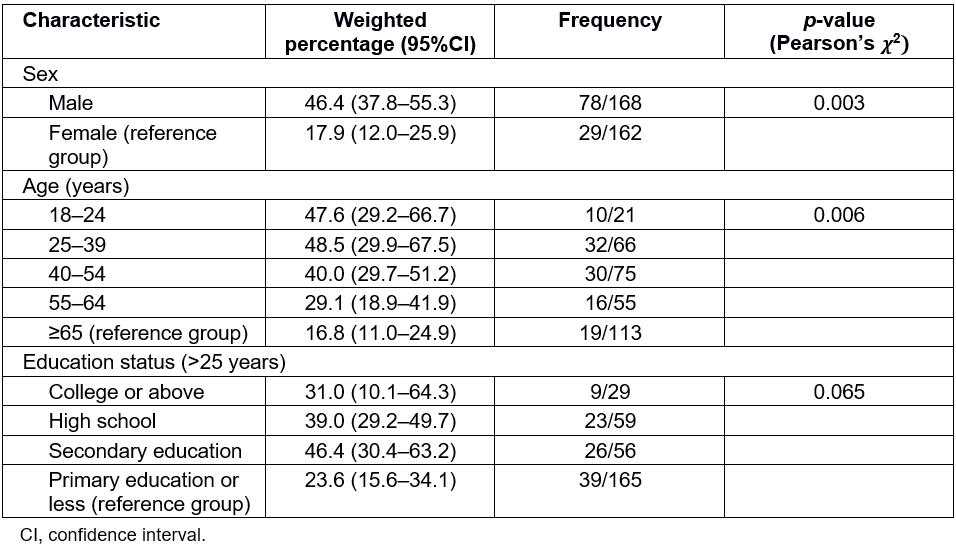
Table 4: Demographic characteristics associated with current smoking and exposure to secondhand smoke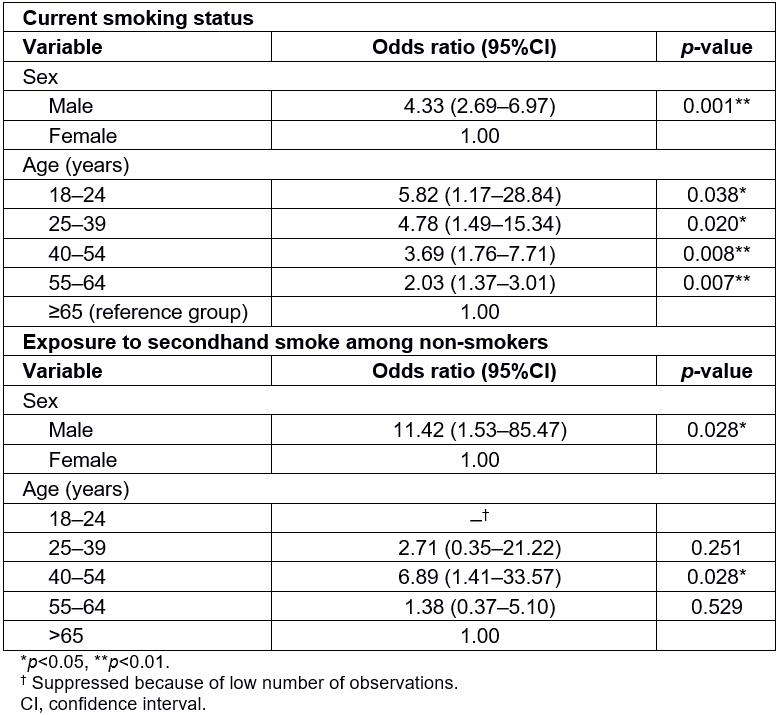
Characteristics of smokers
Daily smokers consumed on average 20.6 cigarettes per day (95%CI 17.67–23.52 cigarettes), which is equal to one pack. Men smoked on a daily basis significantly more cigarettes (23.13, 95%CI 19.20–27.06 cigarettes) in comparison to women (14.04, 95%CI 12.07–16.01 cigarettes; p=0.004).It was noted that nearly seven out of ten (73.2%, 95%CI 63.1–81.4%; 71/97) daily smokers lit their first cigarette of the day within 30 minutes of waking up, indicating high nicotine dependence. The age of initiation was significantly different between men (16.6 years, 95%CI 14.7–18.5 years) and women (21.7 years, 95%CI 18.4–25.0 years; p=0.037). The manufactured cigarette was the most commonly used tobacco product, with only a small number of smokers preferring the hand-rolled one. No use of other tobacco products, including electronic cigarettes, was reported. The average smoker spent €4.20 for each tobacco purchase, usually in the form of cigarette purchase from kiosks.
Smoking cessation
One out of four (25.2%, 95%CI 14.1–41.0%; 27/107) current smokers had attempted to quit smoking during the past 12 months. No one used smoking cessation aids, such as nicotine replacement medication or counseling services. Among all current smokers, 44.9% (95%CI 32.3–58.2%; 48/107) showed no interest in quitting and only 22.5% (95%CI 11.1–40.2%; 24/107) planned to quit during the next 12 months. No statistically significant differences in smoking cessation interest among sex, age groups, education, occupation and marital status were shown.
Secondhand smoke exposure
In only half of the households 49.4% (95%CI 38.7–60.1%) smoking was strictly prohibited and could be considered smoke-free. Overall, 40.4% (95%CI 32.0–49.5%) of the population was exposed to tobacco smoke at home. Furthermore, 62.1% (95%CI 51.7–71.5%; 59/95) of people who worked indoors were exposed to tobacco. It was reported that in more than half of the cases (50.8%, 95%CI 27.8–73.6; 30/59) exposure occurred on a daily basis. No differences in workplace exposure with regards to sex, age, education, marital status or smoking status were shown. High levels of exposure were recorded among those who visited public indoor spaces, especially at restaurants (80.0%, 95%CI 76.0–83.5%; 140/175), bars (87.8%, 95%CI 75.7–94.3%; 79/90), and coffee shops (82.6%, 95%CI 68.4–91.3%; 195/236). Conversely, low exposure was recorded at government buildings, health providers and public transportation.
The Χ2analysis, performed for the population of non-smokers (223 people), showed that more men were exposed to tobacco than women (p=0.015; Table 5). Exposure was very high in the young age groups and low after the age of 55 years. No statistical significance between exposure and other demographics was found. The logistic regression analysis showed that men were 11 times more likely than women to be exposed to smoke (OR 11.42, 95%CI 1.53–85.47; p=0.028) and individuals aged 40–54 years were nearly seven times more likely to be exposed than the oldest group (OR 6.89, 95%CI 1.41–33.57; p=0.028) (Table 4).
Table 5: Prevalence of secondhand exposure of non-smokers by sex, age and highest attained education level
Media and advertising
Overall, 63.6% (95%CI 47.0–77.5%) of the participants noticed anti-smoking information, either about the dangers of smoking or messages encouraging cessation, mainly on television (52.4%, 95%CI 37.0–67.4%) and newspapers (29.7%, 95%CI 21.7–39.2%). On the other hand, cigarette advertisements in stores (12.1%, 95%CI 4.1–30.6%) and logos on clothing or on other items (5.2%, 95%CI 2.8–9.2%) were the only reported pro-tobacco promotion efforts.
Knowledge about smoking harms
Almost all of the participants (96.1%, 95%CI 85.9–99.0%) knew or believed that smoking can cause disease. As shown in Figure 1, the majority acknowledged smoking as an important cause for cardiovascular disease, stroke and lung cancer. Fewer knew that smoking is associated with urinary bladder carcinoma and osteoporosis. Only two out of three participants (67.0%, 95%CI 57.1–75.6%) believed that smoking is responsible for premature death Finally, it was widely known that cigarettes cause addiction (95.8%, 95%CI 90.2–98.2%). The majority of the participants (90.3%; 95%CI 80.0–95.6%) knew that exposure to tobacco can cause harm to adult non-smokers, specifically heart disease, lung cancer and respiratory diseases in children (Fig2). The %uD835%uDF122analysis showed no statistically significant associations between the overall knowledge of harm and demographics or smoking status. Similarly, no association was found between knowledge of harm of environmental tobacco exposure and demographics.
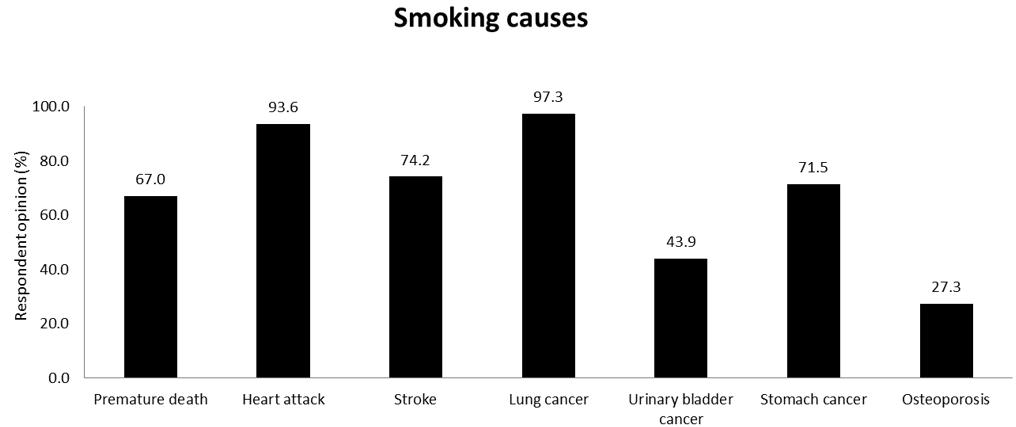 Figure 1: Knowledge about the harms of smoking and exposure to secondhand smoke.
Figure 1: Knowledge about the harms of smoking and exposure to secondhand smoke.
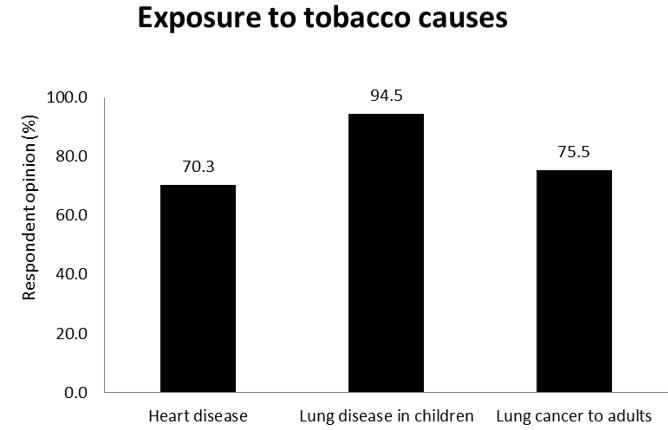 Figure 2: Knowledge about the harms of secondhand exposure to tobacco smoke.
Figure 2: Knowledge about the harms of secondhand exposure to tobacco smoke.
Support of anti-tobacco policies
It was a universally accepted belief that smoking shouldn’t be allowed in hospitals, public transportation, educational institutions (schools, universities) and churches. Respondents strongly supported the laws banning smoking in workplaces (95.2%, 95%CI 93.5–96.4%). Support was associated with current smoking status; more non-smokers compared to smokers supported the prohibitions in workplaces (p=0.004).Support of smoking policies in restaurants was also very high (83.0%, 95%CI 67.3–92.1%) and was associated with age and current smoking status. More individuals aged more than 65 years (94.6%, 95%CI 87.4–97.8 years) were in favor of policies in hospitality venues compared to the youngest group (65.0%, 95%CI 38.9–84.4%; p=0.003). Significantly less smokers supported the prohibitions (65.4%, 95%CI 30.6–89.0% vs 92.7%, 95%CI 85.9–96.4%, respectively; p=0.003). Finally, support of anti-tobacco policies in bars was significantly lower (77.6%, 95%CI 65.7–86.2%) among the population.
Discussion
Main findings
In summary, 46.4% of men and 17.9% of women were current smokers and the overall prevalence of smoking in the area was 32.4%. The bivariate analysis showed that smoking was also common among young adults and graduates of secondary education. Furthermore, high exposure to environmental tobacco smoke was recorded at home, the workplace and in many public spaces. The multivariate analysis showed that being male and young were significant determinants for smoking status, while only sex was the single most significant factor affecting secondhand smoke exposure of non-smokers. Respondents were well informed, although differences in knowledge of tobacco harm existed. No advertising or promotion efforts were reported.
Patterns of smoking
Smoking prevalence is lower than the reported prevalence of the rural part of GATS Greece (38.7%). This difference could be partly attributed to differences in study methodology (age of participation, sampling frame and methodology), but it is also consistent with the downward trend in prevalence as it was previously reported by the Hellas Health surveys9,12. The major differences in smoking patterns between men and women were in prevalence, consumption and age of initiation. Male predominance of smoking is a well documented fact. The low prevalence of smoking among women could be attributed to social bias, as smoking is considered socially unacceptable for women in this rural area. In the study sample more men smoked, consumed more cigarettes and became daily smokers at an earlier age. A similar pattern among men was also reported by Birmpili et al in a northern Greek rural area13. Conversely, women in the study sample smoked less and started later, which indicates that minor differences among rural regions may exist.
Alarmingly, smoking was very common among the young, especially between the ages of 18 and 39 years. This puts young adults at high risk of smoking-related disease and underlines the need for anti-tobacco interventions targeting this group. On the other hand, a sharp decrease of prevalence after the age of 55 years was noted. A comparative analysis of consecutive results of the Hellas Health study showed that the intention to quit smoking was increased among rural residents and persons older than 54 years 14. Additionally, older smokers are more likely to quit smoking due to current or in fear of future health issues compared to other reasons, such as family pressure15. Given that many chronic diseases, such as hypertension and cardiovascular disease, become clinically apparent after the age of 50 years16, the authors speculate that this could also be the case for observations in the present study.
Education was not a significant predictor of current smoking. This finding is in line with previous workplace-based17-19 and population studies20-22. It is well known that smoking use is more prevalent among people with less education23; however, a universal pattern of smoking use does not exist. This finding could be explained by the high smoking prevalence in the general population of Greece, and also by the absence of adequate structures for a systematic anti-smoking campaign. It is of note that a coherent nationwide anti-smoking campaign implemented in 1978 led to a significant reduction of smoking use in Greece24.
Important information about smokers’ cessation efforts and respective attitudes were collected. The most significant findings were the low number of quit attempts, the total lack of use of cessation aids and the low interest in quitting smoking. The proportion of quit attempts was higher in the study sample (25.2%) than in the one reported by the rural GATS Greece (19.7%), but lower than the reported attempts by Schoretsaniti et al (27.1%)14. As mentioned before, this could indicate the existence of local factors affecting smoking epidemiology. Furthermore, the unsuccessful attempts and the lack of motivation may in part be explained by the high nicotine dependence of the smokers, which is deemed a significant predictor of cessation25.
The lack of use of effective cessation methods comes as no surprise, since Greece belongs to the countries among the European Union with low use of aids26. There is a multitude of reasons commonly reported for this including the cost, lack of trust on their effectiveness, safety concerns26, false beliefs27 or even lack of information about cessation help. Since cessation aids are the cornerstone of helping smokers quit28, this is a matter that needs to be addressed as a part of organized efforts to increase the successful quit rates.
Previous studies imply that there may not be significant differences in the patterns of smoking between urban and rural areas20. Interestingly, the present study showed similar smoking patterns with the rural areas of the GATS study7: more men smoking compared to women, rural residents starting smoking during late adolescence, high cigarette consumption and increased secondhand smoke exposure. Despite minor differences, urban populations seem to follow similar patterns of smoking. However, the present study wasn’t designed to detect differences in smoking between urban and rural areas, thus direct comparisons cannot be made.
Patterns of secondhand smoke exposure
Overall, high exposure to secondhand smoke in indoor public and private spaces was recorded. Although not surprising, communities with high rates of smoking, such as the area under study, also suffer from high rates of exposure to secondhand smoke29. This shows primarily a failure of the anti-tobacco efforts in regards to implementation and compliance with the regulations. Since the implementation of anti-smoking laws in 2010, smoking has been prohibited in all indoor public places in Greece. After that time, exposure in bars, restaurants and workplaces decreased significantly30, but it seems that enforcement eventually weakened, leading to a pre-ban increase7,9,31. In the area under study, local health and administrative authorities need to restart the efforts to implement the regulations.
Exposure in public occurs mainly in hospitality venues, namely bars, coffee shops and restaurants, which are frequented by people of different ages on a daily basis. This comes as no surprise, since previous studies showed similar results7-9, thus these establishments should be the focus of future prevention policies. Nevertheless, it is very encouraging that the frequency of exposure in government, healthcare facilities and schools was very low, showing perhaps that certain anti-tobacco attitudes have become common sense.
The involuntary exposure to smoke in home is relatively high, but less than previously reported rates. The Global Youth Tobacco Survey, conducted in 2004–05, showed that nine out of ten adolescents were exposed at home31. Both the GATS and Hellas Health IV surveys showed an exposure rate of about 60%7,11. Still, overall exposure remains high and needs to be curbed to protect the health of sensitive populations and assist the quit efforts of smokers32.
Knowledge on smoking
It was shown that participants were well informed regarding the health effects of active and passive smoking. Almost all the participants knew very well the links between smoking and addiction, premature death or disease. This is a very important fact from a public health standpoint, showing that the population has received and understood the message of tobacco harm. Nevertheless, information campaigns are still required, since there were important facts not commonly known, such as the association between smoking and osteoporosis. The latter is a very important public health issue among older persons and especially women 33,34. The multiple effects of smoking on health, as a causative agent for multiple diseases, should be highlighted more, in order for the public to understand the importance of early cessation and prevention.
Limitations
This study has several limitations that should be taken into consideration. This was a convenient sample of the population, which is inherently susceptible to bias, although every effort was made to ensure representativeness. Moreover, the participation rate was not very high, especially among the age group 18–24 years, which might affect the overall prevalence and strength of conclusions for this age group. Thus, results are specific to the borough and provide estimates only for the specific population. As a cross-sectional study, data were based on self-report and thus are subject to recall and misclassification bias, particularly by smokers who might identify themselves as occasional smokers or women who don’t report smoking, since it is not socially acceptable.
Impact of the study and future recommendations
This survey is one of the few in Greece focusing on smoking, secondhand exposure and their characteristics in a rural area. The authors identified several patterns with importance to tobacco control strategies: smokers were more likely to be men, young, smoke heavily and daily, started at late adolescence, show increased nicotine dependence and show low interest in quitting. In addition, residents of the area are highly exposed to tobacco smoke in closed indoor spaces, most notably at the workplace and hospitality venues. The study conclusions provide primarily the basis on which to design prevention programs and, second, the baseline for monitoring future trends in the area.
Since policies in the area have not proven effective so far, a new effort is necessaryto reduce smoking prevalence and protect the health of non-smokers. Training of health professionals is an essential component of a cost-effective strategy on smoking cessation35. Consequently, primary care physicians could considerably contribute to the formulation of anti-smoking campaigns targeting rural populations, therefore enhancing Greece’s building capacity to control smoking. In this context, tailored educational interventions (eg workshops) related to smoking prevention and cessation for primary care physicians could be an impactful intervention to reduce smoking rate in rural settings.
Behavioural counseling must also be an integral part of the clinical practice. Rural primary care physicians should ask adults about smoking, inform them of cessation options and encourage them to quit early. Special attention is necessary for adolescents and women who may not feel comfortable reporting smoking. Cessation programs are equally important to assist long-time smokers and promote the use of cessation materials.