

Introduction
Adverse childhood experiences (ACEs) are widely researched household and individual events, experienced by children between birth and 18 years, that have the potential to affect a child’s lifelong health and wellbeing1. Exposure to these traumatic events in childhood may increase an individual’s risk for heart disease, liver disease, diabetes, cancer, depression, or other chronic illnesses later in life2-15. Exposure to ACEs may also increase an individual’s tolerance for risky behaviors, leading to unintended pregnancies; alcohol, smoking, or other substance abuse; intimate partner violence; or suicide2-15. The effects of ACE exposure may also result in an intergenerational cycle of experiences, with the effects of parents’ ACE exposure negatively affecting their children16,17. Outcomes related to ACE exposure can have notable and damaging personal consequences, as well as societal consequences that potentially affect use and costs in the employment and workforce, and in the healthcare, mental health, and judicial systems1,16-20. Characterizing ACEs among all populations is an important step to identifying appropriate prevention and intervention efforts.
Research examining the prevalence and patterns of ACEs specifically in rural communities is limited. One published brief focused on ACE exposure among adults from 11 US states, as reported in data from the Behavioral Risk Factor Surveillance System (BRFSS)21. This research found that almost 57% of rural residents reported experiencing at least one ACE in childhood, and 14.6% reported experiencing four or more ACEs; however, the odds of exposure to four or more ACEs were similar for both rural and urban residents21. This same research found a similar rank order for types of ACEs across rural and urban participants and concluded overall that rural and urban residents bore similar burdens of ACE exposure21. The 2011-2012 National Survey of Children’s Health surveyed parents about their children’s exposure to a slightly different list of ACE questions, including one related to economic insecurity22. This survey found that a higher proportion of children from rural areas experienced at least one ACE compared to their urban counterparts22. The same report found that children from rural areas were more likely than their urban counterparts to experience selected ACEs (parental divorce or separation, incarceration of a parent, domestic violence, or living with someone who is mentally ill or has a problem with drugs or alcohol), and for all children, this study found that increasing household incomes were associated with decreased ACE exposure22.
Care coordination, social support services, and access to health care are limited in rural areas23. Thus, families in rural areas may be less equipped to mitigate and manage the effects of ACEs. With almost 13 million children living in rural areas across the USA and with rural areas experiencing higher levels of poverty, higher levels of child maltreatment, and overall lower life expectancies than their urban counterparts, the assessment of ACEs in rural communities is important22-28.
ACE exposure among rural southern residents has yet to be investigated. South Carolina (SC) is representative of the traditional South: it has a much higher rate of African-American residents (27.9% vs 12.6%, p<0.01) and a higher proportion of rural residents (33.7% vs 19.3%, p<0.01) than the rest of the country29. These characteristics are shared by many southern states. Thus, the present study aimed to examine rural–urban differences in the types and counts of ACEs among SC residents and assess for any predictors of ACE exposure among rural residents. Based on previous research using BRFSS data to examine rural–urban differences in ACE exposure21, the authors anticipated that ACE exposure among rural residents would be notable and that the burden of ACE exposure would be similar to that of urban SC residents. Also based on previous research, we expected that race, ethnicity, income, and educational status would predict ACE exposure among SC residents2,30.
Methods
Data source
Using the 2014–2015 BRFSS, a cross-sectional analysis of self-reported ACEs was conducted among respondents from SC. The US Centers for Disease Control and Prevention (CDC) developed and oversees administration of the BRFSS nationwide. The survey collects information on chronic conditions and health-related risk behaviors by state31. The South Carolina Department of Health and Environmental Control (DHEC) manages the administration of the BRFSS, and the University of South Carolina’s Institute of Public Service and Policy Research administers the survey for the state of South Carolina. The survey is conducted daily and uses random digit dialing of landlines and cell phones to reach non-institutionalized adults aged 18 years or more.
In 2014, Children’s Trust of South Carolina, a non-profit organization focused on the prevention of child maltreatment and promotion of child wellbeing, partnered with DHEC to collect 11 questions related to ACEs via the BRFSS30. The ACE questions provided data on type and number of ACEs reported by a survey respondent; however, the survey did not obtain data related to the frequency or severity of any specific ACE. Questions related to ACEs were included in the 2014 and 2015 surveys30.
The BRFSS was administered to 22 634 SC adults in 2014–2015; 19 843 participants agreed to answer the ACE questions used for this study (Table 1). The sample was restricted to 18 176 participants with complete demographic information. Population weights were assigned to each survey respondent by the CDC to correct for under- or oversampling and non-response or non-coverage30.
Table 1: Adverse child experience questions included in the South Carolina Behavioral Risk Factor Surveillance System, 2014–2015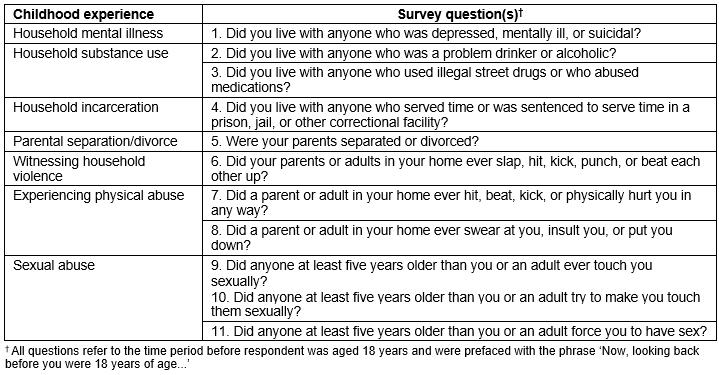
Variable construction
The primary exposure of interest was the geographic residence of each respondent, classified into one of two categories, rural or urban, based on county of residence. South Carolina BRFSS analysts determined the rural or urban status of each respondent prior to releasing the data using self-reported counties cross-walked with urban influence codes (UICs)32. Metropolitan counties (UICs 1, 2) were characterized as urban; micropolitan, small adjacent, and remote rural counties (UICs 3-12) were considered rural.
The primary outcome of interest was overall ACE exposure prior to 18 years. Consistent with previous work on ACEs by rurality21, overall ACE exposure was determined by collapsing overall counts of ACEs into two categories: respondent reports of experiencing fewer than four ACEs (ie 0–4 ACEs) and four or more ACEs. The category of four or more ACEs was used because collective adverse experiences have been associated with poorer collective outcomes33-35.
Covariates included selected sociodemographic characteristics: sex, age, race/ethnicity, educational attainment, and income level. Race and ethnicity were self-reported and grouped into four categories: non-Hispanic white, non-Hispanic black, Hispanic, and other non-Hispanic. Authors grouped age at survey response into seven categories: 18–29, 30–39, 40–49, 50–59, 60–69, 70–79, and 80 years and above. Educational attainment was collapsed into two categories: less than or equal to high school diploma/General Educational Development and at least some college. Income was measured using four categories: less than $25,000, $25,000–49,999, $50,000 or greater, and ‘don’t know/missing’.
Analytic methods
Standard descriptive statistics were used to report frequencies and proportions for each categorical variable. Bivariate analyses assessed for statistical differences between variables, including differences in types and counts of ACEs by rural or urban geographic residence, using χ2 tests, which were considered significant at α=0.05. Multivariable regression models were used to examine the impact of residential rurality and selected sociodemographic characteristics on overall and specific types of ACE exposure. All analyses used survey sampling weights that accounted for the sampling strategy used by the BRFSS study.
Statistical Analytical Software v9 was used for the analyses (SAS; http://www.sas.com).
Ethics approval
The study was approved by the University of South Carolina’s Institutional Review Board as exempt under protocol number Pro00058520.
Results
Demographic findings
For weighted results, the majority of the sample was urban (84.1%), female (52.8%), non-Hispanic white (68.1%), and had at least some college (55.3%, Table 2). Approximately 35.2% of respondents were aged less than 40 years; 51.0% of respondents were between the ages of 40 and 69 years; 14.0% were aged 70 years or more. Over a third (35.2%) of respondents reported an annual income of $50,000 or more. Based on responses to BRFSS questions, the majority of the respondents self-reported that they were in good health (81.3%) and had low to moderate mental distress (86.7%).
In bivariate analysis, rural respondents (15.9% of the overall sample) were more likely to be non-white, less educated, and poorer than their urban counterparts. Over a third (34.9%) of rural respondents reported their race as non-Hispanic black compared to 23.3% of urban respondents (p<0.01). Rural respondents were less likely to have at least some college than their urban counterparts (45.8% vs 57.1%, p<0.01) and were less likely to report incomes of $50,000 or more (26.3% versus 36.9%, p<0.01). Compared to urban respondents, a larger proportion of rural respondents reported poor health (23.9% vs 17.5%, p<0.01).
Table 2: Characteristics of South Carolina Behavioral Risk Factor Surveillance System respondents who participated in the adverse child experiences module of questions, by rurality, 2014–2015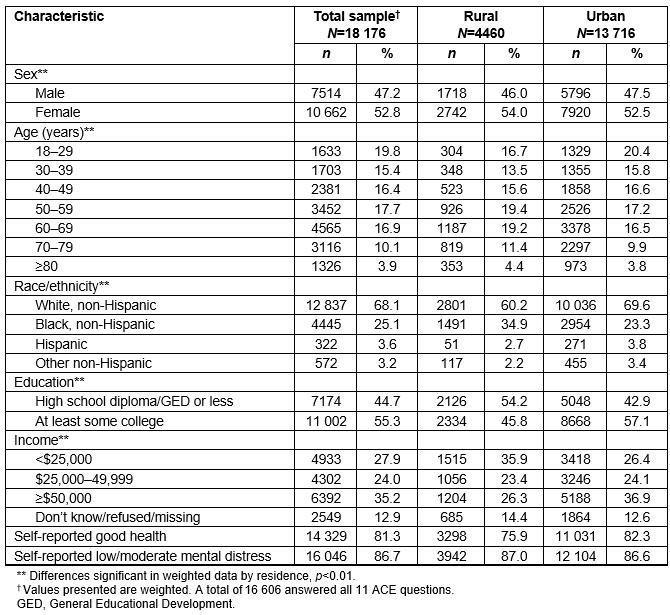
ACEs findings
Among all SC respondents, 61.2% reported experiencing at least one ACE, and 38.7% reported experiencing no ACEs; 44% reported one to three ACEs, and 17.2% reported four or more ACEs. Among all respondents, the top three reported ACEs were parental divorce/separation (30%), emotional abuse (29.6%), and household misuse of alcohol (24.7%). A total of 10.4% of all respondents reported that someone at least 5 years older had touched them sexually.
Rural–urban differences existed for overall ACE exposure. More rural respondents (41.4%) than urban respondents (38.3%) reported not experiencing an ACE (p<0.01, Table 3). Over half (58.6%) of all rural respondents reported at least one ACE compared to 61.7% of all urban respondents (p<0.01). Examining the highest category of ACE exposure, 15.0% of rural respondents reported experiencing four or more ACEs compared to 17.6% of urban respondents (p<0.01).
Rural–urban differences also existed for the types of ACEs. Fewer rural respondents experienced each type of ACE than their urban counterparts. For example, a smaller percentage of rural respondents reported experiencing household mental illness (living with anyone who was depressed, mentally ill, or suicidal) compared to urban respondents (12.6% vs 16.6%, p<0.01, Table 3). Only 9.1% of rural respondents reported living with anyone who used illegal street drugs or abused prescription medications compared to 11.8% of urban respondents (p<0.01). Rural residents also reported lower rates of household incarceration, parental separation/divorce, household domestic violence, and physical, emotional, and sexual abuse.
In logistic regression predicting overall ACE exposure (whether a respondent had four or more ACEs) and adjusting for sex, age, race/ethnicity, education, and income, rural respondents were less likely than urban respondents to report four or more ACEs (adjusted odds ratio (aOR) 0.75, 95% confidence interval (CI) 0.74–0.75, Table 4). Other factors associated with reporting four or more ACEs were sex, age, race/ethnicity, education, and income. The odds of reporting four or more ACEs were higher for female than for male respondents (aOR 1.59, 95%CI 1.58–1.60). Respondents aged 30–39 years were more likely to report four or more ACEs than those aged 18–29 years (aOR 1.11, 95%CI 1.11–1.12). Non-Hispanic blacks were less likely to report four or more ACEs (aOR 0.49, 95%CI 0.48–0.49) than non-Hispanic white respondents. Hispanic respondents also had lower odds of reporting four or more ACEs than non-Hispanic white respondents (aOR 0.44, 95%CI 0.43–0.45). Having at least some college was associated with a lower risk of reporting four or more ACEs compared to respondents who had a high school degree or less (aOR 0.82, 95%CI 0.82–0.82). Finally, higher levels of income were associated with a lower odds of reporting multiple ACEs, with the odds of reporting four or more ACEs lower for those earning $50,000 or more annually (aOR 0.45, 95%CI 0.45–0.45).
Table 3: Types and numbers of adverse child experiences reported by respondents to the South Carolina Behavioral Risk Factor Surveillance System, by rurality, 2014–1015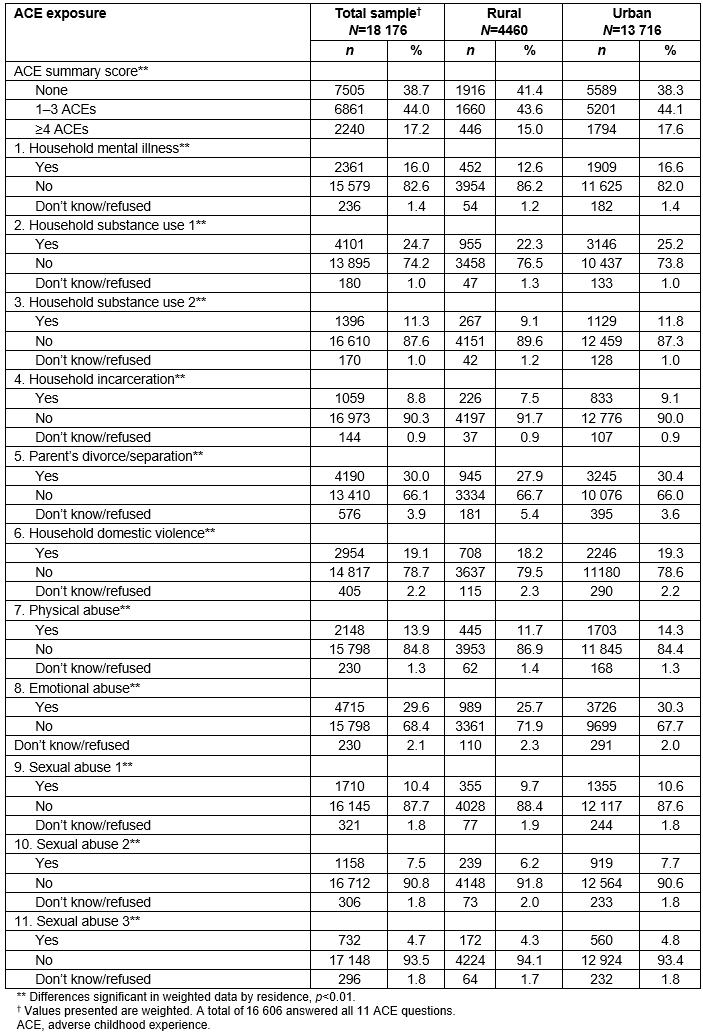
Table 4: Overall adverse child experience exposure reported by South Carolina Behavioral Risk Factor Surveillance System respondents, by rurality and other selected characteristics, 2014–2015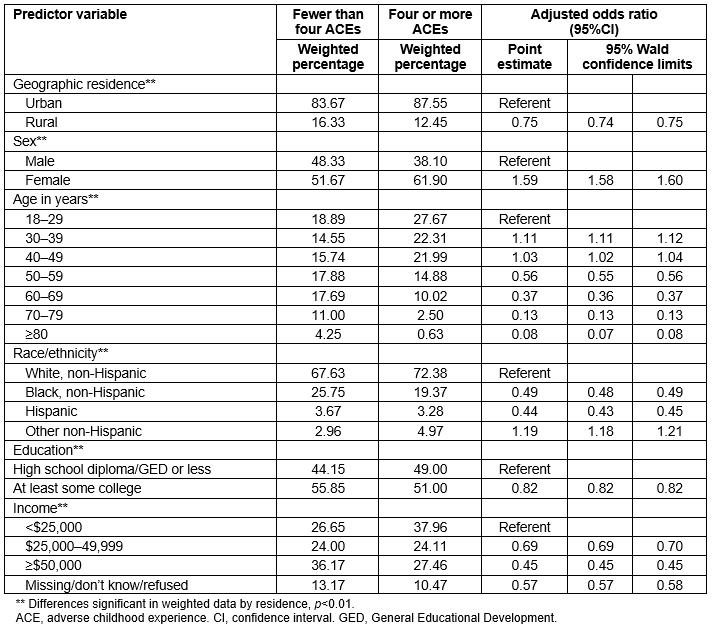
Discussion
This study describes the prevalence and patterns of ACE exposure among rural SC residents who responded to a 2014–2015 BRFSS survey. The results provide new insight into the ACE burden borne by adults in the South, as the study focused on rural–urban differences in ACE exposure in a representative southern state. Overall, 58.6% of rural SC residents reported experiencing at least one ACE. This is a slightly higher proportion than the aggregate numbers reported among rural residents in both a multi-state report based on BRFSS data (56.5%)21 and a report based on National Survey of Children’s Health (NSCH) data (large rural 54.8%; small rural 53.0%)22. The fact that almost 60% of rural residents in SC experienced at least one ACE highlights the need to address this statewide public health issue.
However, compared to their urban counterparts, rural respondents in SC were less likely to report exposure to one to three ACEs, less likely to report exposure to four or more ACEs, and less likely to report each type of ACE. In contrast, previous research using BRFSS data found that ACE exposures did not differ significantly by rural or urban geographic residence21.
The present findings that rural residents of SC report slightly lower exposure to ACEs than their urban counterparts are not wholly unexpected. The 2011–2012 NSCH reported that a higher percentage of children living in rural areas shared meals daily with their families and were more likely to live in safe and supportive community environments than their urban counterparts22. Parents living in rural areas also reported lower levels of parental stress than parents living in urban areas22. In contrast to urban residents, rural residents may experience more social connections within their families and communities22. ‘Social connections’ is one of the five critical protective factors that can support and strengthen families and thus increase positive child development and decrease the likelihood of child maltreatment36.
Consistent with previous work21, the rank order of types of ACEs for both rural and urban SC residents was similar. Among SC respondents, the top three reported ACEs for both rural and urban residents were identical: parental divorce/separation, emotional abuse, and household misuse of alcohol. An earlier study reported the same three top-reported ACEs for both rural and urban residents; however, that study’s combined category of household misuse of alcohol or drugs topped their list for both rural and urban residents21. Also, consistent with previous literature31, across all SC respondents, higher education levels and higher yearly income were associated with lower likelihood of experiencing four or more ACEs.
Strengths and limitations
A limitation among all studies examining ACEs using BRFSS data is that adults are retrospectively reporting their exposure to ACEs. Although these retrospective responses may introduce response bias, the likelihood is greater that responses include more false negatives than false positives, thus resulting in an underestimation of ACE exposure37. A second limitation of this study is that the role of residence based on current residence was examined, rather than residence at the time of the adverse event, and collapsed categories of rural and urban designation are reported, which may mask actual differences in ACE experience by geographic location. Also, the study is limited by the fact that BRFSS does not include institutionalized adults in their survey process. These individuals may have experienced ACEs disproportionally and thus introduce additional bias into the findings. Finally, as a cross-sectional study, no statements can be made on causality, and as a state-specific report, the findings may only be generalizable to similar southern states.
One strength of this study was the use of new ACE data nested in the SC BRFSS survey that allowed access to a relatively large sample size previously unexamined in terms of ACEs. A second strength was the stratification of results by geographic residence, especially in light of the paucity and mixed results of previous work related to ACEs in rural areas.
Public health implications
Although rural respondents may report slightly lower exposure to ACEs than their urban counterparts, the prevalence of ACEs was still notable among rural residents in SC. Thus, the present findings highlight the importance of reaching families and children currently living in rural communities with ACE-related awareness and prevention messages and services. These types of messages are important as the communications can include information on the impact of ACEs, effect of ACEs on child development, importance of positive parenting, and how to build child and family resilience. Additionally, ACE-related awareness and prevention messages can incorporate information on local programs and services that reinforce the content of the communications.
In addressing ACEs in rural SC communities, one barrier may be the typically reduced access to care and services in rural areas38. Residents of rural areas may have limited access to social, mental, medical, or public health services, as well as limited access to transportation to reach those services. Children in rural communities may only encounter child-serving agencies at school, with the children who most need the help not attending school regularly38. This may be one area well suited for policy interventions aimed at increasing availability of local programs and services and access to programs and services that cannot be made available in rural communities.
Researchers have suggested improving parenting skills as one means of reducing ACE exposure in children and have called on pediatricians to engage in this effort, including advocating for an assessment for ACE exposure as part of any comprehensive pediatric medical exam39,40. However, despite having equal access to health insurance, children in rural areas are less likely to have received a preventative healthcare visit in the past 12 months than urban children22 and thus may be less likely to access routine preventative care. Targeted efforts are needed to increase availability and access to parenting skills programs and pediatric care in rural communities.
Others suggest that reducing childhood exposure to adverse and traumatic events requires an integrated, multidisciplinary response16,17. One means of reaching rural families with ACE messages may be through two-generational programs, where children receive early childhood educational services and parents receive training in child development and parenting skills, as well as support that promotes educational attainment and economic sufficiency41. Two-generational programs have been shown to result in better individual outcomes through improving the competencies and support services for caregivers of at-risk children while promoting child-focused development42.
One such example of two-generational programs is the evidence-based home visiting models currently implemented in SC. Many evidence-based home visiting models have been shown to reduce child abuse and neglect through positively influencing parental engagement and improving healthcare usage and child development43,44. In addition to reducing child maltreatment, home visiting programs may reach families that might not otherwise access support services45. Ensuring that evidence-based home visiting models extend their outreach into rural communities may be one important step to reaching rural families with ACE-related messaging and prevention strategies.
Conclusions
Further research on the topic of ACEs in SC will be important to a deeper understanding of this complex issue. Topics important for future research could include an examination of ACEs in rural communities in terms of individuals’ health outcomes and their access to health care, as well as the role of protective factors.
The findings of this study are important because they provide evidence that targeted interventions to prevent exposure to ACEs are just as needed in rural as they are in urban communities. With rural respondents reporting high exposures to adverse events as children, and with rural communities having less access to health and support services, future policies and programs that assist in the prevention of ACEs through targeted outreach and messaging into rural SC are necessary.
Acknowledgements
The authors thank Chelsea Lynes of the Division of Surveillance, Office of Public Health Statistics and Information Services at the South Carolina Department of Health and Environmental Services, for her help and expertise with data acquisition.
This project was supported in part by Children’s Trust of South Carolina; South Carolina Department of Health and Environmental Control; and US Department of Health and Human Services, Administration for Children and Families, Community-Based Child Abuse Prevention grants.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of Children’s Trust of South Carolina, South Carolina Department of Health and Environmental Control, or US Department of Health and Human Services, Administration for Children and Families.