

Introduction
Geriatric assessment has a robust evidence base for improving physical function not only in inpatient settings1 but also in outpatient settings2. Multidimensional assessment of falls risks can prevent falls in older patients3 and falls clinics are an increasingly available outpatient option4. In the Australian health-care context, specialist assessment of cognitive loss is necessary before subsidised cholinesterase inhibitors can be prescribed. Ensuring access to these limited specialist and often multidisciplinary interventions for older adults is a challenge for the health-care system in the context of an increasing population demand. This challenge is even greater in rural or remote areas with the added complexity of distance and declining health workforce.
Outreach services from hospital outpatients' departments are one mechanism for dealing with limited specialist rural services. Four different types of services have been proposed5. The simplest form is the substituted outpatient model which simply moves the hospital clinic to a new location. The replacement model replaces the primary care practitioner with the specialist. Finally, more complex models such as the consultation model or liaison attachment model, where the specialist service is integrated into the primary care environment, have been described6-10.
The Fleurieu region of South Australia is one of the fastest growing regions in Australia in terms of an older population. The hub of the Fleurieu region is 90 km south of Adelaide, the state capital, and covers an area in excess of 2800 km2. The region is home to more than 34 000 people and 22% of the region's population is aged 65 years or more11, compared with 13% nationally12. A map of the Fleurieu region is shown (Fig 1). Older people in the Fleurieu have to travel to Adelaide to access specialist multidisciplinary balance, dementia, and aged care services. For frail older patients, especially those in residential aged care, this journey is arduous.
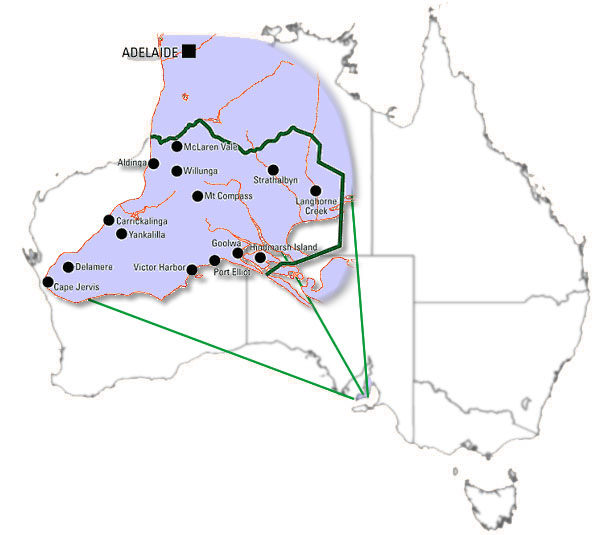
Figure 1: Fleurieu region of South Australia.
Prior to the commencement of this study there was no visiting specialist service in geriatric medicine consulting in the Fleurieu. This was an opportunity to engage with the local allied health and general practitioners to develop a model of care that suited their environment and supported health-care providers in the provision of best care. Therefore, the aim of this study was to develop a model of service delivery, which was feasible in rural environment and delivered specialised falls and memory clinics similar to those available in southern Adelaide. At the end of the first 20 months we wished to evaluate this service in terms of patient access and the satisfaction of the local health-care providers.
Methods
Clinic establishment
A meeting with key stakeholders was held in December 2001 to identify existing service provision in the region and determine which services the new clinic needed to provide. The meeting was attended by six GPs and four allied health professionals. This information was then used to determine the structure of the outreach clinic.
Clinic evaluation
After the clinic was established, a demographic profile of clinic attendees and referral patterns were collected for the next 20 months. Clinical letters were audited to identify what services the clinic had provided to the attendees, including referrals to allied health services, prescription of cholinesterase inhibitors and osteoporosis treatment. After establishing the clinic we assessed patient access, by comparing 3 months of new referrals to the outreach clinic from the Fleurieu region to referrals to our urban based memory and falls clinic in the same period. Patient cancellations on the day of the clinic and failure to attend the appointment were also compared for the calendar year of 2004.
Questionnaires regarding the first year of operation of the outreach clinic were sent to all GPs and members of the multidisciplinary allied health community in the Fleurieu region. These questionnaires included questions about satisfaction with the referral process and whether the clinic had met their patients' needs. The GPs were also able to provide feedback about the nature of the communication they had received from the clinic.
Ethical approval for the establishment of the clinic and data collection was gained from both the Department of Veterans' Affairs Human Research Ethics Committee and the Research and Ethics Committee of the Repatriation General Hospital.
Results
Feedback from the stakeholder meeting informed us that the Fleurieu region had a large number of busy general practices often staffed with practice nurses. Allied health services were delivered by a variety of providers, including the local state-funded health service, private providers, and a day therapy centre as part of a Commonwealth-funded aged care facility.
As is common to health services where all agencies receive funding from different sources and methods, there were problems of integration and some duplication of services. One of the local strategies to deal with this was a fortnightly case conference with all the local providers, health service staff and aged care facilities, where cases and referrals could be coordinated. This group did not have direct GP representation.
GPs identified patients with memory loss and falls and balance problems as the two most important assessments they felt their patients needed.
With regard to what was needed from the proposed outreach clinic, three themes emerged from the stakeholder meeting. These were communication, collaboration and continuing education. For GPs, communication back from the clinic was important because they felt they had an important role in coordinating care. They were often frustrated by specialists who would refer on without discussing this with the GP, because such referrals had often already been made. Similarly, they preferred to manage as far as possible changes to medication, or to be involved in such discussions. Effective communication between GPs, community health-care providers and the outreach clinic was seen as an integral part of any model development. The importance of timely collaboration between clinic staff and community health-care providers was also highlighted. Finally, the need for access to continuing professional development for GPs and community based health professionals was identified.
From this feedback the following clinic model was established:
- The outreach clinic was staffed by a specialist geriatrician and an extended practice nurse (EPN) specialising in aged care.
- The EPN conducted a comprehensive geriatric assessment over approximately one hour, assessing physical function, cognition, and balance, depending on the patient's needs. The EPN attended the clinic fortnightly and the geriatrician would then review the cases referred monthly. The EPN would then arrange referrals to other local allied health services if the need for additional therapy was identified.
- The clinic was designed to provide a service which mirrored the memory clinics and the falls and balance clinic established in southern Adelaide. However, because the outreach clinic did not have the resources to provide the exercise program that is provided in the falls clinic in southern Adelaide13, we referred clients to local providers for any exercise interventions required. This model is similar to a consultation liaison model employed in psychiatry in rural areas5.
- GP communication strategies included the following:
- No patient was seen without a referral from his or her GP. Any cases identified as being suitable for assessment by the EPN at the case conference were first discussed with the client's GP, and referral for assessment was suggested with the final decision left to the GP.
- All GPs received a letter from the specialist regarding the outcome of the assessment.
- If medication changes were planned for previously prescribed medications then these changes were not initiated by the specialist, instead the patient was asked to discuss it first with their GP, after the GP had received the specialist's letter. The only exception to this was cholinesterase inhibitor medications for Alzheimer's disease which were initiated by the specialist.
- No patient was seen without a referral from his or her GP. Any cases identified as being suitable for assessment by the EPN at the case conference were first discussed with the client's GP, and referral for assessment was suggested with the final decision left to the GP.
- To enhance local collaboration, the following strategies were put in place:
- We met with the local public and private allied-health providers on a regular basis and used these professionals as our main source of therapy.
- The clinic was co-located with the local Fleurieu Health Service to allow the EPN to attend the already established fortnightly multidisciplinary case conference. In addition, the team would visit residents in the local aged care facilities as required.
- If a client required admission to hospital or was admitted to hospital, the EPN facilitated liaison between the allied health team and the hospital.
- Our continuing education strategy consisted of a range of educational sessions for local service providers.
- We met with the local public and private allied-health providers on a regular basis and used these professionals as our main source of therapy.
Demographic profile of the outreach clinic attendees
Between May 2003 and December 2004, 115 people were seen by the EPN. Of these, 106 were seen at the outreach clinic, six patients seen in residential care facilities and three seen as inpatients in the local hospital. The average age of clients was 79.9 years (range 50 to 94). A total of 62 (53.9%) were referred for assessment of cognition, 51 people (44.3%) were referred for balance problems, a specialist review for another problem was requested for 20 people (17.4%), a specific review of the patients medication for five people (4.3%) and nursing home visits, largely for behavioural disturbance, in six people (5.2%).
Examination of referrals to the service showed 99 patients (86.1%) were referred for only one problem and 16 for multiple problems. The most common combination was for assessments of cognition and balance, and two patients were referred for assessment of balance, cognition, specific medication review, and another medical problem requiring specialist review.
Outcomes of clinic attendance
There were a total of 99 letters available for analysis out of the 115 patients seen by the EPN. Table 1 shows the recommendations made to the GP for patients referred for either balance problems or cognition problems, and for all referrals analysed extracted from available clinic letters. Letters were not available for clients who were seen in a residential care facility because the letter was hand-written in the resident's notes.
Table 1: Outcome of attendances to the outreach clinic (patients may have been referred for more than one type)
Patient access
Table 2 outlines the patient access data for the outreach clinic and the equivalent clinics in southern Adelaide. All patients have a considerable wait to see the specialist both in urban and rural areas, although wait times in the Fleurieu clinic were slightly longer than for comparable Adelaide clinics. The average time to see the EPN was 40.1 days, shorter than the wait time to see a specialist in any of the three clinics considered. Failure to attend for the appointment was similar for each clinic.
Table 2: Patient access data from the clinic
GP questionnaire
A questionnaire concerning the outreach clinic was sent to referring GPs, and nine responses from 23 GPs (39%) were received. All respondents reported the clinic was useful, that referrals contributed to the management of the clients, and the clinic provided the service expected. When asked what was helpful about the outreach clinic, responses included satisfaction with the services provided, appreciation of the availability of further opinion/support for their patients, and that the clinic improved access to other specialist services at the southern Adelaide hospital. Overall, the GPs supported the clinic's continuance.
Allied health questionnaire
A questionnaire concerning the presence of the EPN at the Fleurieu region multidisciplinary team meetings was distributed to the 14 allied-health team members who attended the meetings. There were 11 respondents (79%) from a range of disciplines including nursing, social work, and occupational therapy. They represented different agencies, including aged-care providers, community rehabilitation providers, and community health staff from the South Australian Department of Health.
The clinic was well received by all allied health respondents, with all indicating that it was a useful service that provided the service expected, and they found the liaison service to local allied-health providers valuable. All responded that attendance by the EPN at the multidisciplinary meetings added value to the meetings, contributed to the care of the clients presented at the meetings, and provided options for care. Allied-health workers noted that clients not seen at the outreach clinic also benefited from the EPN's attendance at the multidisciplinary meetings. The two main aspects of the clinic that were noted as useful by the allied health workers were: (i) outreach clinic members' integration into the local provider network; and (ii) regular attendance by the EPN, regardless of whether referral of a client had been made or not, improved uptake of the clinic in the community.
Some suggestions to improve the clinic were made, including:
- the ability for allied-health workers to make direct referrals to the clinic, instead of having to go through a GP
- access to a copy of the letter from the clinic geriatrician to the client's GP be made to relevant treating members of the local health service, in order to be up to date with client care.
Discussion
Although the concept of urban-based specialists travelling to other areas to provide health services is not new, the success of such services has not been reported widely. We are reporting the results of a geriatric clinic focussing on the problems of cognitive and balance assessment. The currently available literature describes a range of services including psychiatry14, oncology15,and a range of surgical specialties16 but often without details of the access or outcomes of the services delivered. In this study, we used a hybrid 'consultation liaison' model5 which worked in tandem with the local health service providers. Integrating with the local health service was a critical factor in identifying local residents most in need of assessment. By firstly consulting with local health-care providers to identify the needs of the rural community, we were able to develop a model of service that fulfilled the needs of the community that was acceptable to all. We have demonstrated that the model we developed and integrated into the local health service could be a viable model for other rural communities. It is robust enough to service more remote areas even when allowing for the travel required.
The available randomised controlled trials for outreach clinics have suggested a range of health benefits including improved symptom control for depression17, reduced use of diagnostic tests18 and improved adherence to treatment guidelines for breast cancer19. In a similar way, there was a wide range of interventions suggested to clients after attendance at our clinic. In particular, there were suggestions regarding evidence-based strategies related to falls and injury prevention, including vitamin D supplementation20 and exercise21. Patients were able to access cholinesterase inhibitors for Alzheimer's disease as well as to receive advice about guardianship and other issues related to dementia. A surprising number of clients received advice about ongoing driving, including at least three patients whose licences were suspended. This is an important but difficult health issue for patients with dementia, and a visiting cognition service can play a role in assisting GPs.
Previously reported benefits of establishing outreach clinics include reduced travel time and shorter waiting lists for attendees to that service22. A recent systematic review14 showed that specialist outreach clinics in the rural setting can improve access, outcomes and service use, but that better quality evidence concerning the effects of specialist outreach in the rural sector is needed. In our clinic we were able to achieve some of those outcomes. Our waiting times for assessment by the specialist were not better than in comparable clinics in southern Adelaide. The available consulting time and the community demand for the service drives waiting times for clinics and, in our case, given the long waits the demand outstripped the available resources. Although we used an EPN to carry out many of the assessments that ordinarily a medical practitioner would do, this did not compensate for the lack of available medical workforce. The 'failure to attend' rate was not better in the rural location. We had hypothesised that shorter travel times would lead to better patient attendance as seen other studies23 but this was not borne out in our study. Unfortunately using our available data we were not able to show better access to the clinic by moving it to Victor Harbor. Indeed, this clinic was performing as a 'substituted outpatients', with the trade-off being probable greater convenience for the local population versus the increased cost of travel for the clinic staff, similar to experience in the UK24. However many of the patients assessed (in particular those in an aged care facility) would not have been able to travel to Adelaide and, hence, we did improve access for these local residents. Furthermore, the local health-care workers may not have felt comfortable suggesting to the local GP a patient review in Adelaide, but were comfortable requesting this review locally. Unfortunately we were not able to directly compare patient satisfaction with our metropolitan clinic with the rural clinic. Arguably this information would have provided the best evidence that the rural clinic increased access to the services offered, by making them available in their local area.
Outreach models provide advantages for local providers and consumers, and are particularly useful for diagnostic services and non-emergency speciality care for patients with chronic diseases16. Benefits for health-care providers in the local area may include the shared workload, reduced professional isolation, increased capacity to manage complex cases locally, and an improved reputation of local services. Although the number of GP respondents was low, the GPs surveyed reflected on some of these themes (including one who commented on the usefulness of assessment even though little actual change could occur for the patient), thus improving their certainty in managing a complex case. The clinic has offered advantages to local providers, as evidenced in our study, and was a valuable support to both the local health service and the surrounding GPs. One GP commented that the ability to access all the services in one clinic was an advantage. We are aware that dementia assessment services are available in some rural parts of Australia but our service was able to provide other assessments relevant to ageing, in particular falls and balance.
Our intervention was not without its limitations, however, when we compare to the performance of the falls clinic in Adelaide13. In an urban falls clinic, 34% of attending patients underwent a bone density test while none of our clients had this test recommended. Similarly, 89% of urban falls clinic clients had some sort of exercise recommendation as opposed to 41.9% in our clinic. This was due to the unavailability of bone densitometry and reduced allied-health services in this area. The urban falls clinic had funding built in for an exercise intervention whereas, in the rural setting, this was not possible and local services were alone available. This is a major limitation of the current model since so many of the recommendations rely on the presence of other services to be instituted. New creative solutions are needed to deal with these workforce limitations. One potential solution would be to train our nurses to deliver a home-based exercise program similar to the method developed in New Zealand25. In the final analysis, while our rural clinic model was not as well resourced as its metropolitan equivalent, it did provide an improvement on the previous lack of locally available service.
While our clinic model is a possible mechanism for delivering ambulatory aged-care services to rural and remote regions, this model of care does not guarantee improved access and shorter waiting times for attendees. Available resources including adequate funding, allied health and nursing time limited our clinic model. Future models of rural care may need to address innovative workforce strategies to improve access.
Acknowledgements
This project was funded by a grant from the Department of Veterans' Affairs. We would like to thank Ms Jackie Stepien-Hulleman for her assistance with the manuscript preparation.
References
1. Stuck AE, Siu AL, Wieland GD, Adams J, Rubenstein LZ. Comprehensive geriatric assessment: a meta-analysis of controlled trials. Lancet 1993; 342(8878): 1032-1036.
2. Cohen HJ, Fuessner JR, Weinberger M et al. A controlled trial of inpatient and outpatient geriatric evaluation and management. New England Journal of Medicine 2002; 346: 905-912.
3. Tinetti ME, Baker DI, McAvay G et al. A multifactorial intervention to reduce the risk of falling among elderly people living in the community. New England Journal of Medicine 1994; 331: 821-827.
4. Hill K, Smith R, Schwarz J. Falls Clinics in Australia: A survey of current practice, and recommendations for future development. Australian Health Review 2001; 24: 163-174.
5. Cord-Udy N. The medical specialist outreach assistance program in South Australia. Australasian Psychiatry 2003; 11: 189-194.
6. Mitchell AR. Psychiatrists in primary health care settings. British Journal of Psychiatry 1985; 147: 371-379.
7. Strathdee G, Williams P. A survey of psychiatrists in primary care: the silent growth of a new service. Journal of the Royal College of General Practitioners 1984; 34: 615-618.
8. Tyrer P, Ferguson B, Wadsworth J. Liaison psychiatry in general practice: the comprehensive collaborative model. Acta Psychiatrica Scandanavica 1990; 81: 359-363.
9. Williams P, Clare A. Changing patterns of psychiatric care. BMJ 1981; 282: 375-377.
10. Bower P, Gask L. The changing nature of consultation-liaison in primary care: bridging the gap between research and practice. General Hospital Psychiatry 2002; 24: 63-70.
11. Australian Bureau of Statistics. Regional Statistics South Australia. Canberra, 2003.
12. Australian Bureau of Statistics. Year book Australia. Canberra: ABS, 2004.
13. Houghton S, Birks V, Whitehead C, Crotty M. Experience of a falls and injuries risk assessment clinic over two years. Australian Health Review 2004; 28: 374-381.
14. Gruen RL, Weeramanthri TS, Knight SE, Bailie RS. Specialist outreach clinics in primary care and rural hospital settings. Cochrane Database of Systematic Reviews 2004; (3): CD 003798.
15. Smith SM, Campbell NC. Provision of oncology services in remote rural areas: A Scottish perspective. European Journal of Cancer Care 2004; 13: 185-192.
16. Tracy R, Saltzman KL, Wakefield DS. Considerations in establishing visiting consultant clinics in rural hospital communities. Hospital and Health Services Administration 1996; 41: 255-265.
17. Katon W, Von Korff M, Lin E, Simon G, Walker E, Bush T. Collaborative treatment to achieve treatment guidelines. Impact on depression on primary care. JAMA 1995; 273: 1026-1031.
18. Vierhout WP, Knottnerus JA, van Ooij A, Crebolder HF, Pop P, Wesslingh-Megans AM. Effectiveness of joint consultation sessions of general practitioners and orthopaedic surgeons for locomotor system disorders. Lancet 1995; 346(8981): 990-994.
19. Howe HL, Lehnherr M, Katterhagen JG. Effects of physician outreach programs on rural urban differences in breast cancer management. Journal of Rural Health 1997; 13: 109-117.
20. Chapuy M, Arlot M, Duboeuf F et al. Vitamin D and calcium to prevent hip fractures in elderly women. New England Journal of Medicine1992; 327: 1637-1642.
21. American Geriatrics Society BGSAAoOS. Guideline for the prevention of falls in older persons. Journal of the American Geriatrics Society 2001; 49: 664-672.
22. Bowling A, Stramer K, Dickinson E, Windsor J, Bond M. Evaluation of specialists' outreach clinics in general practice in England: process and acceptability to patients, specialists, and general practitioners. Journal of Epidemiology and Community Health 1997; 51: 52-61.
23. O'Brien K, Mattick R, Mandall N, Wright J, Conboy F, Gosden T. Are specialised outreach clinics for orthodontic consultation effective? British Dental Journal 2001; 158: 1638-1644.
24. Powell J. Systematic review of outreach clinics in primary care in the UK. Journal of Health Services Research Policy 2002; 7: 177-183.
25. Campbell AJ, Robertson MC, Gardner MM, Norton RN, Tilyard MW, Buchner DM. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ 1997; 315(7115): 1065-1069.