



Introduction
Primary healthcare (PHC) professionals should recognize pathological internet use in their everyday practice1-3. Raising their awareness on cyber-safety seems to be a new challenge in their continuing educational agenda, aiming to increase their competency to early detect and confront pathological practices or refer people for specialist care4.
Since 2010, the funding of healthcare services in Greece has been severely reduced, especially affecting rural and remote communities5. During this austerity period, rural PHC professionals have requested guidance on the management of issues they struggle to cope with due to reduced quality and equity in health care6. The development and implementation of low-cost interventions, based on volunteerism, that introduce PHC professionals’ training and their involvement as educators in school-based interventions in their communities have not been previously tested internationally. This study aimed to explore the experiences and level of awareness on cyber-safety among PHC professionals, who were trained and encouraged to serve as educators in a school-based intervention on safe internet use.
Methods
Study design
All directors of the 18 PHC centers of the Third Health Authority (prefecture of Macedonia, Greece) were asked to invite their personnel to participate in the project7,8. The participants attended a 1-day train-the-trainers course and were encouraged to become educators in their communities’ schools. No special incentives were given to increase participation.
Primary healthcare professionals’ training
On September 2013, participants attended a 7-hour course on social networks, online gaming, cyber-gambling, cyber-bullying, internet addiction, including informative websites about cyber-safety and ways to report illegal cyber-activities. Additionally, they practiced on leading a school-class discussion, in small groups. The context of the discussion was pre-defined in order to ensure homogeneity in delivering the intervention.
The training curriculum was developed and delivered by PHC professionals, specializing in cyber-safety, and an expert trainer. The involvement of PHC professionals ensured that it would be appropriate for the PHC context, while the expert adjusted it to the students’ needs. A specialist police officer was also included as a trainer.
School-based intervention
Schools were selected using a multistage stratified random sampling technique, according to the location (urban/semi-urban/rural) and school grade level (middle, school and high school – aged 12–18 years)7. The school visits were performed in October and November of 2013. Upon distributing the Internet Addiction Test7,9,10, the PHC professionals proceeded to the 30-minute intervention until the end of the school hour (usual length 45 min). Children’s guardians were informed 3 days in advance and provided their written informed consent.
The pre-defined agenda included use of social networks and ‘friends’ in Facebook, amount of time spent online and reliability of internet information. Additionally, the educators wrote on the class-boards the name of a website with reliable information about cyber-safety and one that is a hotline for reporting illegal cyber-content, and the phone number of the helpline YpoSTIRIZO (Greek Safer Internet Center).
Evaluation of the educators’ experiences
One month after the school intervention, all participants completed voluntarily and anonymously an 11-item evaluation questionnaire, developed for the needs of this study. They were asked to return it by mail, in order to ensure anonymity. It comprised questions about professional background, previous experience in school-based interventions and open-ended questions on likes or dislikes, possible problems and willingness to participate in future projects.
Data analysis
Continuous variables were summarized with mean and standard deviation. Categorical variables were presented with frequencies and the corresponding percentages. All analyses were performed with the Statistics Package for the Social Sciences v24.0 (IBM; http://www.spss.com). Open-ended questions were analyzed using thematic content analysis11. Analysis began with open coding. Using comparison across the answers, the open codes were refined into major themes, until saturation was reached. The final themes were agreed upon after two researchers (ZT and AD) reached consensus.
Ethics approval
Approval from the Greek Ministry of Education and Religion was obtained (reference number 91243/Γ2/08.07.13).
Results
Description of participants
Thirteen PHC centers participated (response rate 72.2%), while five responded negatively because of lack of personnel. PHC personnel were informed, asking for a maximum of 10% to participate, and 51 of 577 professionals (8.8% response rate) volunteered. Six (11.1%) didn’t ultimately accept the role of educators because of time constrains. The 46 educators visited a total of 30 middle schools and 21 high schools, reaching 8053 students (1811 (22.5%) from urban areas, 2924 (36.3%) from semi-urban areas and 3318 (41.2%) from rural areas). Their characteristics are presented in Table 1.
Table 1: Primary healthcare professionals’ characteristics (n=46)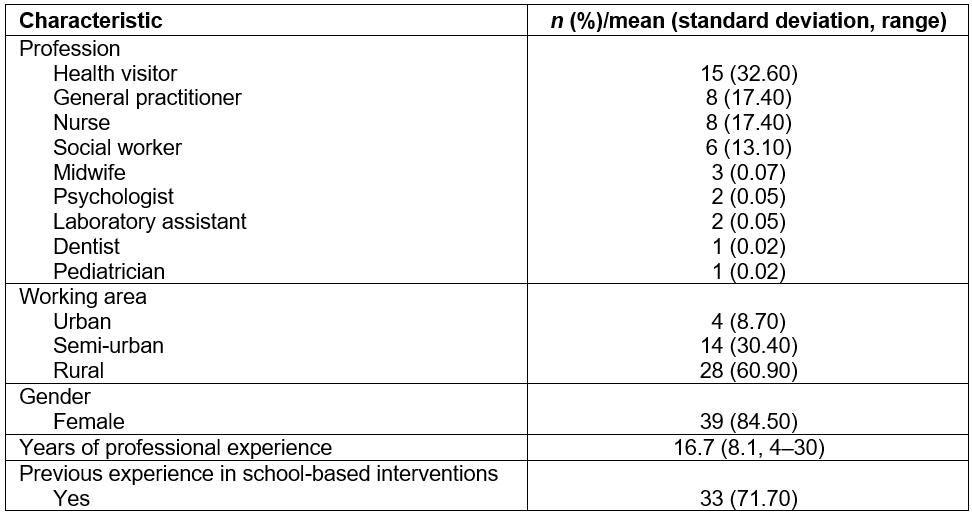
Evaluation
All 46 educators positively evaluated their experience, recognizing gains that can be summarized in four main themes: (i) acquisition of new knowledge on cyber-safety, (ii) ethical reward for their contribution in raising awareness in students, (iii) revitalizing effect of the interaction with youth and (iv) re-enforcement of cooperation and team spirit. Quotes describing each theme are presented in Table 2. Only two professionals made negative comments, both concerning their out-of-pocket travel expenses to schools.
All 46 educators declared their willingness to participate in future projects with students, 29 (63.4%) wanted to inform parents, while 11 (24.4%) were interested in training teachers.
Table 2: Benefits of project participation identified by primary healthcare professionals, across four themes
Discussion
This article reports on the experience of PHC professionals trained in order to serve as educators in the first (to our knowledge) multi-center, school-based, PHC professional-led intervention on cyber-safety in adolescents. The professionals recognized numerous gains, further emphasized by their enthusiasm to participate in future health promotion projects.
Because of the novelty of this project, it is difficult to compare these findings with previous literature. There are no previous studies on PHC professionals as trained educators for health promotion among school children. Studies among adolescents in peer leadership prevention programs have reported positive effects on peer educators themselves12,13. Moreover, train-the-trainer programs among Australian health professionals have reported effectiveness in enhancing practice in rural and remote settings14. Personal enrichment and optimism in teaching the subject they have been trained on was also reported in faculty members of South African health sciences institutions15. The acquisition of new knowledge, the ethical reward for raising awareness in adolescents, the revitalizing effect of the interaction with youth and the enforcement of cooperation were the main gains recognized by the participants. Interestingly, these gains have outweighed the absence of incentives and the out-of-pocket payment of the participants’ transfer expenses to schools.
During the austerity period, PHC researchers were urged to focus on how to implement cost-effective interventions16. Although this project was designed and implemented by volunteers, ensuring its low cost, it has already provided evidence of its effectiveness in raising awareness in the attending students8. Moreover, the findings suggest that the combination of the trainee and the trainer’s experience of the PCH professionals was effective in increasing their understanding and therefore raising their awareness of cyber-safety, providing both a satisfying and rewarding experience. It would be useful to further explore whether the participants have included cyber-safety in their practice and whether they had the capacity to counsel, prevent and early detect pathological internet use. Moreover, it would be interesting to investigate if similar health promotion interventions by health professionals could be applied in other cultures.
Among the limitations of this study is that the findings are based on self-reported answers and therefore possible response bias should be considered in interpretation. Investigation of experiences through open-ended questions instead of a comprehensive interview may have restricted the amount and quality of provided information. In order to minimize the effect of bias, by ensuring anonymity, the voluntary completion of an evaluation questionnaire was preferred over the possibly more informative personal interviews or focus groups, where the participants might have hesitated to reply honestly. Furthermore, the questionnaire was a low-cost and convenient method to collect data from a large number of people in distant geographical locations. Another issue is that the evaluation of the train-the-trainer course wasn’t carried out directly after its completion and therefore an evaluation of the course alone is not available. Overall feedback was obtained 1 month after the completion of the intervention, and that could possibly involve a recall bias. However, this choice was made in order to capture the impact that the whole project (the combination of being a trainee and a trainer) would have on the participants, after a small period of time that would enable them to reflect on their entire experience.
Conclusions
The experience of participation in the train-the-trainers course and the subsequent school-based intervention was very highly evaluated by the participants, who recognized numerous gains. The involvement of trained PHC providers as educators in the schools of their communities is a promising method in raising their own awareness, especially on new topics that should be included in their continuous educational agenda. It was low in cost, since it was designed and implemented by volunteers, but large in scale. This project emphasizes the crucial role that PHC professionals can play in health promotion not only through practices in their offices, but also in their communities’ schools in urban, semi-urban, rural and remote areas.
Acknowledgements
We thank the 46 PHC professionals who were involved with enthusiasm in this study and all the students and teachers who participated. We would like to specially thank Dr George Kormas for all his guidance and precious help in developing the training curriculum for this intervention and training the healthcare professionals educators.