

Introduction
Regular participation in physical activity across the lifespan is a recommended strategy for the prevention of diabetes and other chronic diseases1. Health disparities between Aboriginal and non-Aboriginal Australians commence in childhood: Aboriginal children experience rates of type 2 diabetes six times higher than those of non-Aboriginal children2. The Australian physical activity recommendations for children aged 5–17 years advise accumulation of at least 60 minutes per day of moderate-to-vigorous physical activity (MVPA)3. Physical activity participation across multiple contexts and settings is necessary to ensure children meet national recommendations4, and patterns of physical activity may vary according to season5 and on weekdays versus weekends6. Organised physical activity, including sports clubs, provide an important organised setting for physical activity4,7. Children’s physical activity also occurs outside organised settings, including the period after school8 and during active commuting to/from school9.
Global declines in physical activity prior to the period of adolescence are evident and have been demonstrated to commence in children aged as young as 7 years10. In Australia, the New South Wales (NSW) Schools Physical Activity and Nutrition Survey (SPANS) observed decreases in the proportion of children meeting physical activity recommendations between 2004 and 201511,12. Physical activity declines may be particularly pronounced in rural settings where children in general are known to be less active than in urban areas13 and where higher proportions of Aboriginal children reside, relative to urban areas14.
Children’s participation in regular physical activity is strongly influenced by individual and environmental barriers. This is well established in non-Aboriginal populations where commonly reported barriers include a lack of time15, availability and suitability of activities16, affordability as well as neighbourhood and home safety, travel distances, weather and parental influence17. Studies of barriers involving remote-dwelling Aboriginal participants, which are rare, suggest ‘shame’ or being deeply self-conscious of being physically active are barriers that negatively influence participation in both Aboriginal and Torres Strait Islander (Australia’s other Indigenous population) people18,19. A further study in a rural/regional area of Australia found that Aboriginal young people described various environmental barriers such as transport to facilities, poor amenities and aesthetics (visual aspects)20.
A recent cross-sectional study, using validated measures, found low levels of overall physical activity in a sample of Aboriginal children21. National cross-sectional government data highlights that while Aboriginal children aged 5–17 years are more active than their non-Aboriginal counterparts, the reverse is true for adults22. The timing of these age-related changes is unknown, although one study reported that higher levels of physical activity are maintained at ages 10–12 years23. Data from multiple time points are required to better understand physical activity patterns and to assist in identifying critical ages where physical activity promotion may have the greatest impact. Participation across multiple components, or across multiple time points, has yet to be described among Aboriginal children. This study aimed to explore how physical activity patterns varied according to season, setting and type among Aboriginal and non-Aboriginal children in rural NSW, Australia.
Methods
Study details
Participants in this repeated cross-sectional study were Aboriginal and non-Aboriginal children in grades 5, 6, 7 and 8, recruited through all primary (grades 5 and 6; approximate age 10–12 years) and secondary (grades 7 and 8; approximate age 12–14 years) schools in two towns and surrounding communities on the rural north coast of NSW. The current study was part of a larger study, the Many Rivers Diabetes Prevention Project (MRDPP), which has been reported elsewhere24,25. The two towns have populations sizes of 14 000 and 25 000 respectively, are in a coastal region with an abundance of rivers and a subtropical climate26 and have higher than the national proportions27 of Aboriginal people, at 19% and 8%, respectively28. Both areas are classified as inner regional areas on the Australian Standard Geographical Classification Remoteness Areas measure29 and as being of low socioeconomic status with low Socio%u2010Economic Indexes for Areas (SEIFA) scores representing disadvantage30.
For survey 1 (T1; 2007–2008), children were sampled from all 38 schools (28 NSW Department of Education and Training and 10 independent) in the towns, all of which had both Aboriginal and non-Aboriginal students. For survey 2 (T2; 2011–2012), 36 of the 38 schools that took part in the previous survey elected to participate again; one school had closed and in another only had five eligible children, none of whom consented. Aboriginal project officers (APOs) from the participating communities provided key leadership in managing the information and consent process for all children during the data collection, assisted by casual Aboriginal staff, and participated in data entry and interpretations of results. Further details of the comprehensive Aboriginal community governance processes and structure, led by Aboriginal community controlled health organisations and involving extensive community consultation and capacity building, are available elsewhere25.
Measures
The Many Rivers Physical Activity Recall Questionnaire (MRPARQ) was used to assess the physical activity of the participants at both T1 and T2. This measure was adapted from the Australian Physical Activity Recall Questionnaire31 and has been previously validated in a sample of young people from the communities participating in this study23. Children were asked to record their weekly frequency and duration in different activities in different questionnaire sections and given assistance on which section to place a particular activity where required by APOs and through use of posters with location-specific examples of activity type by organised/non-organised. The MRPARQ sections provide data on 14 different components: organised, non-organised, club, school (other than physical education), travel to/from school, after school and weekend – in both summer and winter. Some of these components were the sum of other components: ‘organised’ comprised club and (organised) school activities and ‘non-organised’ comprised travel to/from school, school (non-organised) after school. The ‘school’ component comprised both the organised (other than physical education) and non-organised school activities and children were asked to record after-school and weekend activity done at these times in these categories exclusively. The MRPARQ also collected information on the sociodemographic variables of self-reported Aboriginal status (Aboriginal v non-Aboriginal), sex (male v female), age in years and school grade (grades 5–8).
Analyses
The normality of the questionnaire data was examined using histograms for each physical activity component as categorical variables. Each component appeared to be normally distributed. Weekly mean minutes and 95% confidence intervals (CIs) at T1 and T2 and change in physical activity for each component from T1 to T2 were calculated using t-tests. Descriptive statistics were used to calculate the proportion meeting Australian recommendations3 at T1 and T2 in the total sample and among Aboriginal and non-Aboriginal children. Children were categorised as meeting (versus not meeting) recommendations if they achieved ≥60 minutes of MVPA and on 7 days of the week. Linear mixed-model regression analysis was used to compare Aboriginal and non-Aboriginal children for change in weekly mean minutes for each of the 14 MRPARQ physical activity components. A stepwise procedure with backward elimination of non-significant interactions and covariates to identify significant moderators and predictors was used for each outcome. The fixed effects in the model were group (Aboriginal and non-Aboriginal), time (baseline and follow-up), sex, school year, group/time interaction and other interaction terms found to be statistically significant at p<0.1. The random effect in the model was school identification, to account for clustering by school. Differences of adjusted mean change and 95%CIs were determined using the linear mixed models. Cohen’s d was used to determine the magnitude of the differences (post-test difference between baseline and follow-up mean minutes/pooled pre-test standard deviation of Aboriginal and non-Aboriginal scores). Analyses were performed using the Statistical Package for the Social Sciences v19.0 (IBM; http://www.spss.com) and SAS software v9.4 (SAS Institute, http://www.sas.com). p<0.05 was considered statistically significant unless otherwise stated.
Ethics approval
The study protocol was approved by the Hunter Area Health Service (06/08/23/4.02; 2006); the Mid North Coast Health Service (360N; 2006); the University of Newcastle (H-357-1206; 2006); the New South Wales (NSW) Department of Education and Training (2006106; 2007); and the Aboriginal Health and Medical Research Council of NSW, Australia (494/05; 2005). Ethics approval was also part of the Aboriginal community governance process. Written informed consent from the parents and the children’s assent were requirements for participation. The study was carried out in accordance with the principles of the Declaration of Helsinki as revised in 2000.
Results
In 2007–2008 (T1), physical activity data were collected from 1545 children, 246 of whom identified as Aboriginal (15.9%), in grades 5–8 at 38 schools (overall response rate 43% of eligible children). The response rate among the Aboriginal children at T1 was 55% (compared with 41% of non-Indigenous children), and 43% of respondents were male. In 2011–2012 (T2), physical activity data were collected from 923 children (240 Aboriginal, 26.0%) in grades 5-8 at 36 schools (overall response rate 29%). The response rate among the Aboriginal children at T2 was 44% of those enrolled (compared with 26% of non-Indigenous children) and 45% of respondents were male. Respondents were aged between 10 and 14 years at each time point, with 28.3% of Aboriginal and 29.0% of non-Aboriginal children aged 11 years at T1 and 39.6% of Aboriginal and 34.1% of non-Aboriginal children aged 11 years at T2. No children completed the survey at both time points. There were fewer male than female respondents among both Aboriginal and non-Aboriginal children. The distributions of age, sex and school year did not differ over time among either group, with the exception of school year among the non-Aboriginal children where there tended to be few children in grades 7–8 at T2 (Table 1).
Among both Aboriginal and non-Aboriginal children, there were overall declines in proportions of children meeting physical activity recommendations from T1 to T2 of 13.2% (summer) and 18.7% (winter) for the Aboriginal children; and 9.6% (summer), 9.4% (winter) for the non-Aboriginal children (all p<0.005, Table 2). There were also declines in weekly mean minutes of travel to/from school (summer and winter) and after-school activity (winter, all p<0.05, Table 3).
Among the Aboriginal children, there were declines in weekly mean minutes of organised (winter) and non-organised (summer and winter) activity (all p<0.05, Table 3). Among the non-Aboriginal children, there were increases in weekly mean minutes in school (summer and winter) and weekend (summer) activity (all p<0.05, Table 3).
There were significant effects of Aboriginal status by time (T1 to T2) for the school (summer and winter, both p<0.001), weekend (summer, p=0.02) and organised (winter, p<0.001) components. In each of these components, there was a mean decline in the activity of the Aboriginal children and a mean increase in the activity of the non-Aboriginal children.
Table 1: Sociodemographic characteristics of the sample by survey year for Aboriginal and non-Aboriginal children 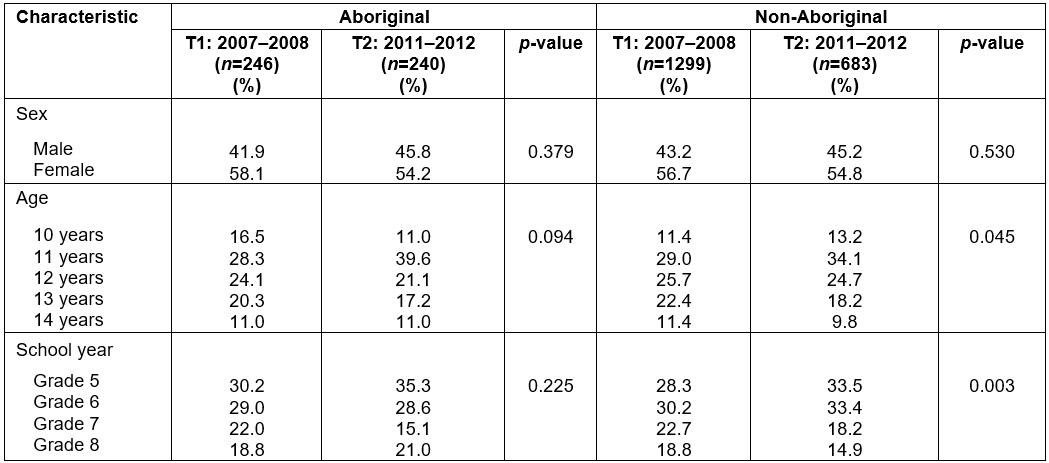
Table 2: Changes in proportions of those meeting physical activity recommendations in both seasons in the whole sample and by Aboriginality
Table 3: Weekly mean minutes and change of physical activity between baseline and follow-up by components, stratified by Aboriginality and adjusted for school clustering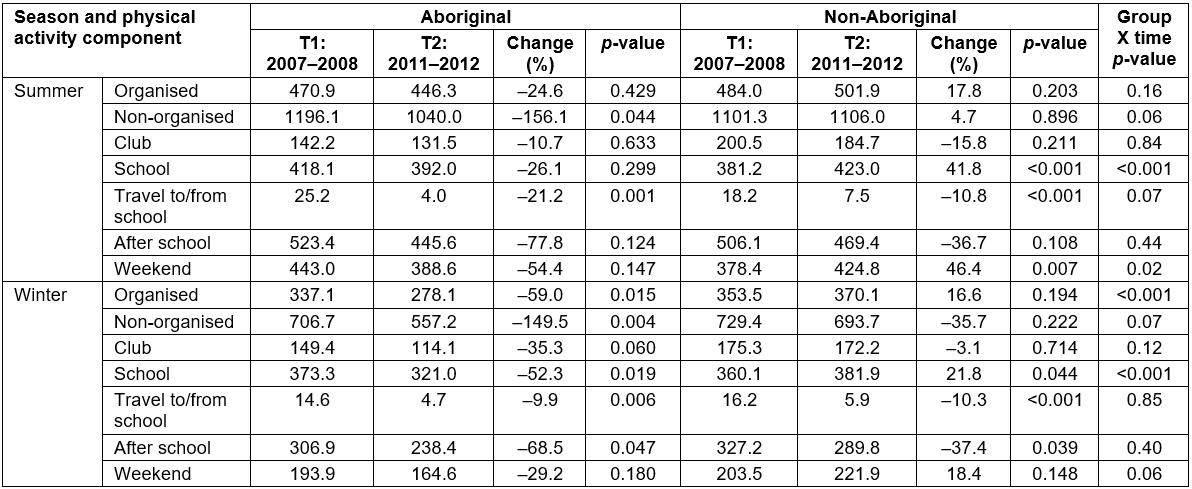
Discussion
Physical activity decreased over time for both Aboriginal and non-Aboriginal children in the study sample. There were variations in weekly minutes of physical activity according to Aboriginal status, season, setting and activity type. Declines in particular components were greater among Aboriginal compared to non-Aboriginal children.
A significant decline was found in the proportion of both Aboriginal and non-Aboriginal children meeting Australian physical activity recommendations. This finding is consistent with a recent study reporting low overall physical activity levels among Aboriginal and non-Aboriginal children21 as well as statewide trends13 over a similar time period. The decline in overall physical activity levels, as well as in a number of specific components, was more notable among Aboriginal children than among their non-Aboriginal counterparts. This was statistically significant for four components: summer school, summer weekend, winter organised and winter school. This finding may be due in part to the lower questionnaire completion rates for non-Aboriginal children in 2011–2012, which may reflect a bias towards families more motivated to make positive health behaviour change. Yet children from disadvantaged communities, such as those in this study sample, are typically less active than their more advantaged counterparts32. Both areas participating in the MRDPP were reported as having a higher proportion of Aboriginal people28 (who experience greater social disadvantage) than the national average. While it would not have been possible to obtain accurate self-reported, individual-level socioeconomic status measures from children as young as 10 years, both areas are classified by the Australian Bureau of Statistics as areas of high relative socioeconomic disadvantage according to the SEIFA30. A further explanation of the more marked declines in physical activity across several components among Aboriginal children may relate to experiences of racism, which is a distinct determinant of health33 and may directly influence physical activity through affecting motivation or opportunities to participate in mainstream group activities24.
International review evidence has found variation in children’s activity between summer and winter, with most studies finding higher activity levels in summer5. Higher activity levels in summer compared to winter were also apparent in both Aboriginal and non-Aboriginal children in the present study, possibly reflecting the particular influence of rural river and subtropical coastal environments in the study sample26. The study did not find significant changes over time, nor differences by Aboriginal status, for organised activity in the summer, or for club activity in either season. While organised activity contributed almost a third of the total physical activity in both seasons and for both groups, activity levels of Aboriginal children in the organised and club components were lower in both seasons and time points than for non-Aboriginal children. The lower levels of club activity among Aboriginal children may reflect factors reported in focus groups conducted with the communities24, which include a lack of transport, racism within the communities and cost (Aboriginal communities possess a lower mean weekly income than their non-Aboriginal counterparts27). Preferences for alternative physical activities such as non-organised outdoor activities have been found to be more appealing and popular among Aboriginal populations34, and the authors postulate that this may be associated with similar reasons to those experienced by the present cohort.
The contribution of organised sport to overall physical activity levels in young people in NSW has been demonstrated previously35. Encouragingly all children in the present sample achieved higher levels of organised physical activity than that of grade 6 and grade 8 students in NSW state data from a similar time period (2010), who achieved 263.2 and 371.0 weekly mean minutes, respectively, averaged across both seasons but through almost identical measures13,24. Nonetheless, participation in both organised and non-organised physical activity is essential to achieving recommendations for health and development among young people34, and strategies to increase participation among Aboriginal children in particular are crucial.
Time spent travelling to and from school significantly declined in both Aboriginal and non-Aboriginal children in summer and winter. While NSW state data for 2010–2015 did not significantly change, active travel rates were low at both time points; for example, only 19.9% and 16.0% of children walked to school in 2010 and 2015, respectively36. National active transportation levels of children are also low as exemplified by a ‘D+’ rating in the recent Australian Report Card on Physical Activity for Children and Youth3. Current low levels can be attributed to automobile transport36. This may have been particularly pertinent in the present study’s rural sample, where greater distances travelled to school can be an additional barrier to active transport. Given established evidence of the benefits of active travel to school9, school and community-led strategies to increase current low levels of active commuting in children are required.
More intensive efforts to specifically target physical activity participation may result in increased activity levels during this critical adolescent time period, where physical activity declines have occurred internationally12 and across NSW in a similar time period and age group13. Physical activity was promoted as part of the MRDPP; however, it was not an intensive component of the intervention relative to nutrition and diabetes knowledge, and this is reflected in the present study’s findings of overall declines. Many programs that aim to increase physical activity for health and social outcomes among Aboriginal adults and children exist37, and community ownership and program delivery by community members is critically important25. The present study’s findings indicate that programs to increase non-organised activity as well as organised and school activity in winter among the Aboriginal children are particularly warranted. Specific recommended approaches include natural resource or land management programs34 or assistance in supporting the cost of organised sport, such as a voucher scheme. However, a greater focus on the broader social and family determinants of health in Aboriginal people and communities, such as education and employment opportunities, along with racism33, is also likely to be necessary in order to have an impact on specific health risk factors. Many of these approaches are likely to similarly benefit low socioeconomic, non-Aboriginal populations and represent a clear policy direction to address inequality.
Limitations of the study include a possible selection bias, given the differential participation rates for Aboriginal (higher) and non-Aboriginal children (lower) and lower participation rates for non-Aboriginal children in 2011–2012 compared to 2007–2008. However, the authors consider that the leadership of the local community APO team was likely a critical factor in achieving higher participation rates among Aboriginal children than non-Aboriginal children, as well as in comparison to statewide surveillance11,12 and should be viewed as a strength of the study. Further strengths include a comparable sample of non-Aboriginal participants from the same regional and low socioeconomic setting. The self-report MRPARQ tool is a robust, established measure, which has been validated with objective measures within a similar population23, and is consistent with existing measures, allowing for comparisons to statewide data.
Conclusions
In this population of Aboriginal and non-Aboriginal children from regional, low-socioeconomic areas, physical activity declines were observed over two time points but not across all types, seasons or settings. Patterns of physical activity differed between Aboriginal and non-Aboriginal children, with lower physical activity levels among Aboriginal children and declines in both summer and winter non-organised, winter-organized and school activity components. More intensive, specific promotion of physical activity in these components is required.
Acknowledgements
The authors acknowledge the traditional owners of the lands on which this program of research and health promotion was conducted, the Biripi and Dunghutti peoples and their elders past and present. We thank them for their guidance and support and for allowing the Many Rivers project to be carried out on their land.
References
You might also be interested in:
2005 - Rabies surveillance in the rural population of Cluj County, Romania