





Introduction
During the preschool years (ages 3–5 years), higher levels of physical activity have been associated with healthy body composition and a range of positive psychosocial health and cognitive outcomes, such as self-regulation and attention1,2. In this age group, early childhood education and care (ECEC) settings play an important role in physical activity3. ECEC settings have been identified as an ideal setting for the facilitation and promotion of physical activity and population-based obesity prevention in young children4-6. Preschool-aged children’s physical activity that takes place in ECEC settings in high-income countries is strongly associated with a number of factors, including age, sex, gross motor skill proficiency, opportunities to be active, outdoor environment characteristics and time spent outdoors5,7. Specifically, boys tend to be more active than girls, children with greater gross motor skill proficiency tend to be more physically active than children with poorer proficiency, and spacious outdoor areas tend to be more conducive to higher levels of physical activity. Other factors, for which the evidence is equivocal, include features of the physical environment (eg open spaces), children’s body mass index or adiposity, and the educators’ presence, training, qualifications, attitudes and behaviours5. Educators in ECEC settings have reported being aware of their role in promoting children’s physical activity, but also aware that they may be a hindrance to physical activity8.
Little is known about physical activity in ECEC settings in low- and middle-income countries, and the factors that affect physical activity in these settings. The ECEC factors that promote or hinder physical activity may operate differently. Recent evidence about rural South African preschool children indicates that preschool children possess skills that could influence physical activity in ECEC settings in rural South Africa. First, rural preschool children have been found to have superior gross motor skills compared to South African preschool children from urban low- and high-income settings9. Second, gross motor skills have been positively associated with cognitive development (specifically executive function) in preschool children from this population10, with South African preschool children (including from rural settings) actually outperforming an age-matched sample from Australia, using the same measure of executive function11. These findings are novel, and in many ways unexpected, so explanations for them are still somewhat speculative. Nevertheless, they do suggest that rural South African children may be developing certain physical and cognitive skills that could potentially influence their ability to benefit from interventions in these settings. However, it is still important to consider the resource-related challenges faced in South Africa, as one of the low- and middle-income countries.
Educators in ECEC settings in low-income South African communities have less (if any) training and inadequate resources, with those in low-income rural communities faring the worst12,13. These resource challenges are acknowledged to have an impact on the promotion of quality opportunities for physical activity and ultimately the health and development of young children14,15. There is limited research identifying potential intervention points targeting physical activity in this age group in South Africa, as well as other low- and middle-income countries. Identifying potential strategies to include in interventions is essential for the planning and implementation of appropriate and feasible physical activity programs in ECEC settings in low- and middle-income countries. It cannot be assumed that interventions developed and implemented in high-income countries (and even in low-income settings) will necessarily be feasible and effective in low- and middle-income countries. Where factors associated with physical activity are identified, these can be included in policies at government and local levels, and targeted in practices within ECEC environments, to support preschool children’s physical activity.
Considering the challenges faced in ECEC settings in low- and middle-income countries, including those in South Africa, it is important to extend understanding of urban ECEC settings in South Africa to include low-income, rural communities. To date, only one study conducted in an urban setting has reported on physical activity in ECEC settings in South Africa16. This study reported that children in the low-income ECEC settings spent significantly more time in MVPA than their higher income peers (11% v 8% of the preschool day, p=0.018), and light-intensity physical activity (LPA) did not differ between income settings (18% and 16% of the preschool day, respectively)16. By understanding physical activity in ECEC settings in a rural community in South Africa, researchers will be able to make comparisons between settings and, if necessary, make evidence-based adaptations to existing interventions that promote and optimise physical activity in both urban and rural ECEC settings. These interventions should both maximise the strengths and appropriately consider the challenges of these settings.
Therefore, within a low-income rural community in South Africa, this study aimed to report on the characteristics of the physical activity environment within ECEC settings and identify child-level and contextual factors associated with physical activity in ECEC settings in a low- and middle-income country.
Methods
This article presents a cross-sectional study conducted in 2014, for which data were analysed between 2016 and 2017. Details of the study setting, sample and methods have been reported elsewhere14. The STROBE checklist for cohort studies was followed in the reporting of this study17.
Study setting, sample and recruitment
The study took place in the Agincourt research area of the Medical Research Council / Wits University’s Rural Health and Transitions Research Unit, Bushbuckridge, Mpumalanga province, which is a low-income rural area in north-eastern South Africa. This area is characterised by a high unemployment rate (29% for men, 46% for women)18, as well as a lack of access to electricity, tarred roads and running water19. Previously published qualitative work from the broader study has reported several perceived barriers (by parents) for children’s participation in physical activity, including crime, lack of facilities and lack of knowledge14. Additionally, parents and teachers report (and the researchers observed) that there are no indoor play spaces or facilities designed for children’s physical activity.
To recruit as many preschool-aged children as possible for this study, primary school reception year (grade R) classes were included as ECEC settings, because some preschool-aged children (particularly aged 5 years) in South Africa attend grade R at primary schools. Three independent preschools and two primary schools were invited to participate. In this context, independent preschools are not private. They receive minimal funding from the government for day-to-day functioning, which does not cover the salaries of staff. Independent preschools in South Africa generally rely on the school fees paid by parents/caregivers. However, the independent preschools included in this study were fortunate to receive monetary donations, which have allowed to them to upgrade the facilities at the preschool. For the purpose of this article, children from preschools are referred to as ‘preschool’ children and primary school children are referred to as ‘grade R’ children.
Parents and caregivers of preschool and grade R children were invited to an information meeting at the ECEC settings to give written, informed consent for their child to participate in the study. Consent was obtained for 131 children. To be consistent with a previous study conducted in South Africa, observation commenced at 8 am and continued for approximately 4 hours throughout the preschool day16. Children for whom consent was received (for the broader project, described in detail elsewhere14) were identified and selected on arrival at the ECEC setting, and the sample therefore included the first 10–14 children who arrived, depending on the ECEC setting (between 10 and 14 observations took place at each of the ECEC settings). Thus, a total of 55 children (23 boys, 32 girls) were selected for observation (33 preschool, 22 grade R).
Data collection
Observational assessment of the physical activity environment: An observational assessment of the environment was adapted from existing tools20-22. The items of each tool that the researchers felt were relevant for rural South Africa were extracted (based on the researchers’ exposure to the preschools and understanding of the context) and used to compile the adapted tool. The tool included items used in other studies that identified different types of equipment, counted equipment and measured space23,24. The tool was split into four different sections: outdoor area, equipment (indoor and outdoor), indoor play space and policy practices. The components (and results) of the outdoor area and equipment are shown in Table 1. The section on indoor play evaluates the space allocated for play and the presence of screens (eg TV, DVDs). The last section, on policies, includes questions on the schedule of the school day, including the allocation of time to free, outdoor and structured play. Policies (if available) pertaining to physical activity were viewed, and previous training of educators on physical activity and/or gross motor skills was noted, based on verbal feedback from staff.
Table 1: Characteristics of the study’s outdoor physical activity environment, by early child education and care setting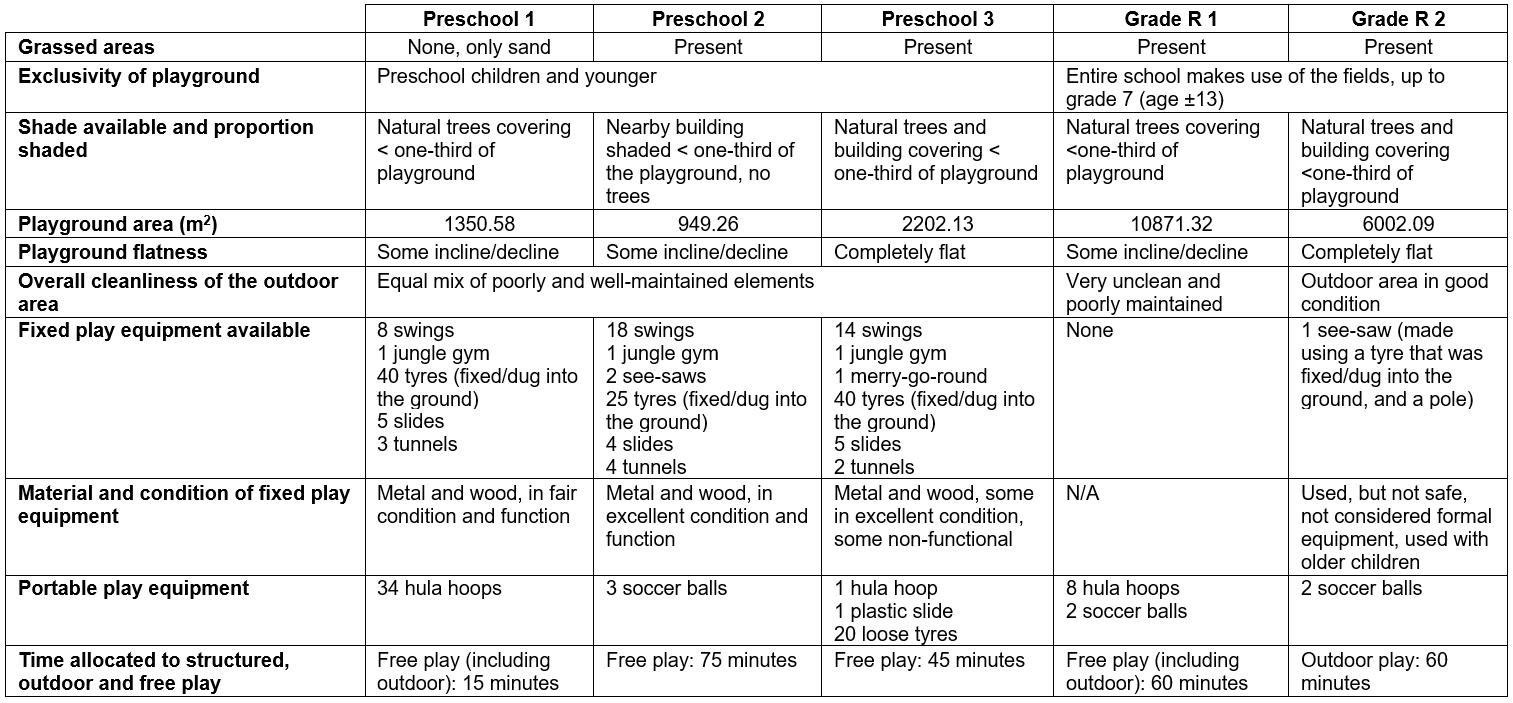
Observation of physical activity: The Observational System for Recording Physical Activity in Children – Preschool Version (OSRAC-P) was used to observe children’s physical activity and sedentary behaviour25. The OSRAC-P includes an extensive list of activities (Fig1) in which preschool-aged children participate and is specific to the preschool environment26. The OSRAC-P observation entails a timed observation of a focal child for 5 seconds, followed by a capturing interval (ordering shown in Fig1). In the present study, this cycle was repeated 30 times per child, after which a different child became the focal point for 30 observations. The Open Data Kit Collect application v1.4.10 (Open Data Kit; http://opendatakit.org/about) was used to electronically capture the OSRAC-P data on a Google Nexus 7 tablet and then exported as an Excel spreadsheet for cleaning and analysis. For components of the data analyses, physical activity level categories in the OSRAC-P were combined: ‘stationary’ and ‘limb movement’ were referred to as sedentary behaviour, ‘slow easy’ was referred to as LPA, and ‘moderate’ and ‘fast’ were referred to as MVPA16,27.
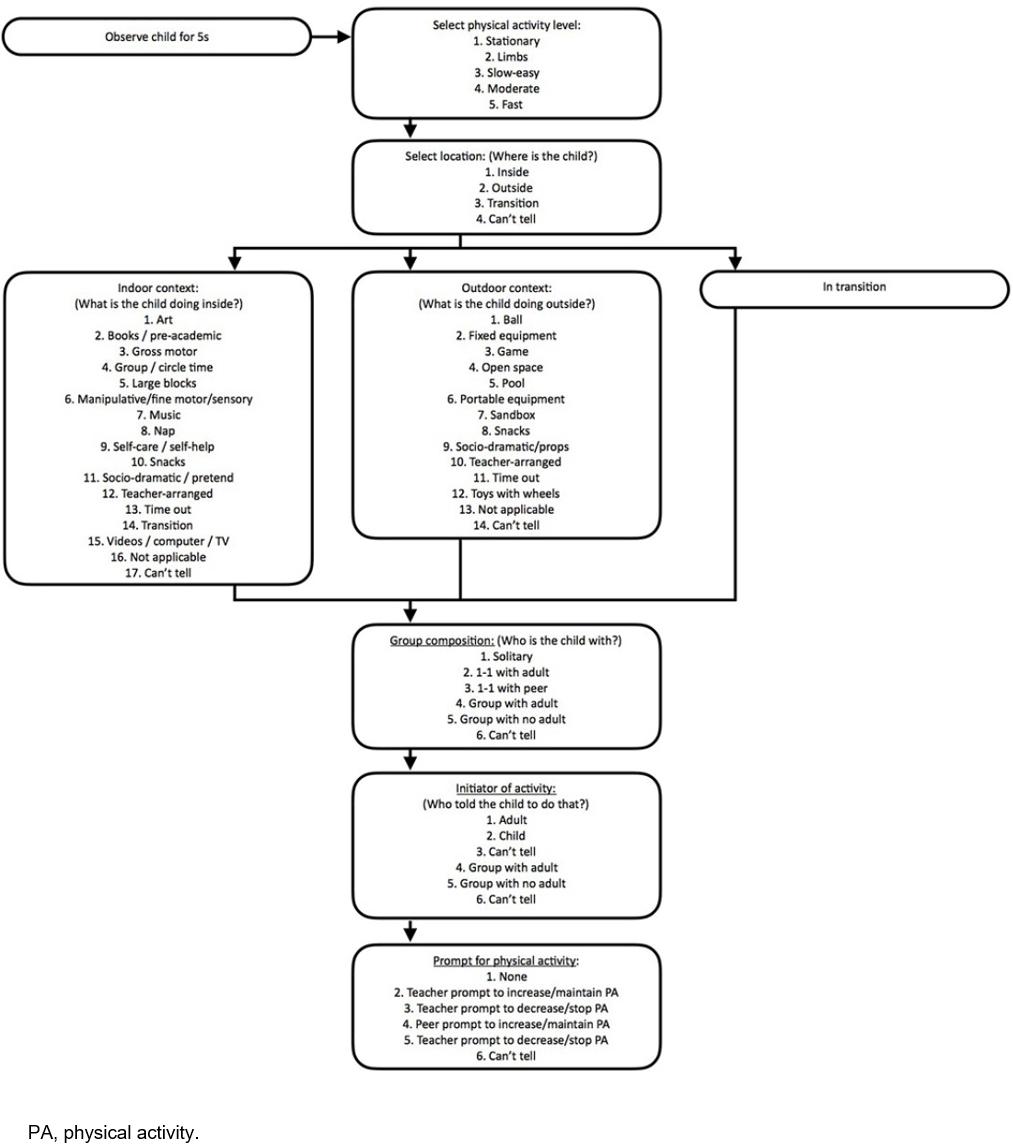 Figure 1: Flow diagram illustrating the coding of activity using the Observational System for Recording Physical Activity in Children – Preschool Version
Figure 1: Flow diagram illustrating the coding of activity using the Observational System for Recording Physical Activity in Children – Preschool Version
Assessment of anthropometrics: Children’s height and weight (shoes and heavy clothing removed) were measured using a portable stadiometer (Leicester 214 Transportable Stadiometer; Seca GmbH & Co, Hamburg, Germany) and a calibrated scale (Soehnle 7840 Mediscale Digital; Soehnle Industrial Solutions GmbH, Backnang, Germany). All measurements were taken twice by author CD for consistency, and an average taken of the two measurements for analysis. For both height and weight, a third measurement was taken if there was a discrepancy of more than 5 mm between the first two measurements, in which case the two closest measurements were averaged. Height and weight were used to calculate body mass index. The International Obesity Task Force cut-offs were used to classify children as ‘thin’, normal weight, overweight, obese or morbidly obese28.
Statistical analysis: Differences in anthropometric data by sex and ECEC setting were assessed using unpaired t-tests for normally distributed data, and Mann–Whitney U-tests for data that were not normally distributed. Descriptive statistics regarding the physical activity environment are presented to compare the five ECEC settings. OSRAC-P data are presented as proportion of time (as a percentage) spent in different physical activity intensities. Pearson’s χ2 analyses were used to determine differences between the ECEC settings (preschool and grade R) for the OSRAC-P variables including proportions of time spent in different physical activity intensities, as well as the contexts of physical activity (Fig1).
A multinomial logistic regression analysis was performed to determine child-level (sex, weight status) and contextual (setting (grade R, preschool), location (inside, outside) and activity initiator) factors associated with LPA and MVPA (with sedentary behaviour as the reference variable) in the ECEC settings. Although playground size, availability of fixed play equipment and number of portable pieces of equipment were assessed, these variables were not included in the regression analysis due to these characteristics being highly related to the preschool and grade R ECEC settings. Thus, ECEC setting (preschool, grade R) was used as a variable, and not the individual characteristics. Stata v13 for Mac (StataCorp; http://www.stata.com) was used to perform all analyses.
Ethics approval
Ethical approval for the study was obtained from the University of Cape Town Human Research Ethics Committee (237/2012), the University of the Witwatersrand (Wits) Human Research Ethics Committee (Medical) (M140250), and the Mpumalanga Provincial Departments of Health and Education. This study adheres to the guidelines described in the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects29.
Results
Sample characteristics
The sample characteristics are shown in Table 2. There were no significant differences between boys and girls, and the only difference between preschool and grade R children was in mean age (grade R children older, 5.6±0.3 years v 4.5±0.4 years; p<0.001).
Table 2: Descriptive characteristics of sample, by sex and setting type†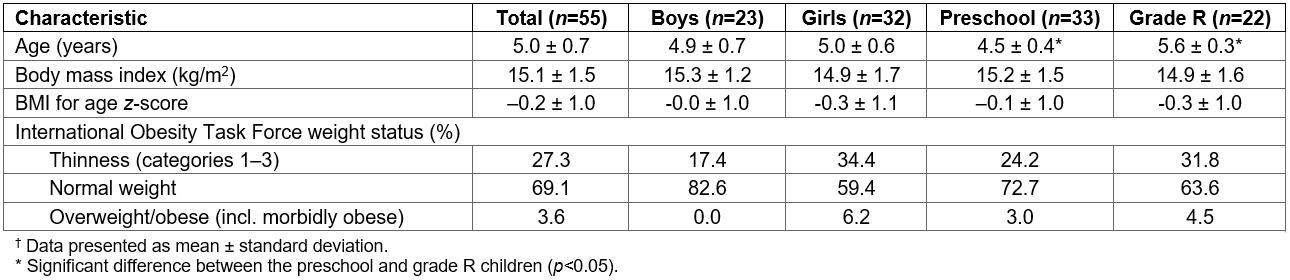
Physical activity environment
The playground sizes and characteristics of the outdoor settings are presented in Table 1. None of the ECEC settings had indoor active play spaces, screens, lesson plans for physical activity, time scheduled for physical education or organised physical activity, or written physical activity policies. None of the ECEC settings provided after-school activities such as ball skills. None of the educators had received training on physical activity or gross motor skills, nor had access to resources informing them of how to promote physical activity or gross motor skills in ECEC settings.
Although the observation of teaching styles and education strategies was not an outcome of the study, it is worth noting that time spent in educational activities (coded as ‘group or circle time’, ‘books, pre-academic, writing, listening, science and math centres and activities’ or ‘manipulative, fine motor and sensory centres and activities’) was mostly in a didactic learning format. It often included rote-learning and reciting back to the teacher (eg letters of the alphabet, days of the week, months of the year). Teachers would stand at the front of a classroom (or group of children) with the children seated. None of the learning was child-led or intentionally play-based.
Observation of physical activity
A total of 1693 OSRAC-P observations were completed (1066 at the preschools, 627 at the grade R settings). Table 3 summarises the proportion of the preschool day (as a percentage) spent in each of the OSRAC-P categories. The greatest proportion of time was spent in sedentary activities (69.9%) and this differed significantly between preschool (63.2%) and grade R children (81.3%, p<0.001). Preschool children participated in significantly more time in LPA (8.6% v 2.7%, p<0.001) and MVPA (25.4% v 15.3%, p<0.001). Preschool children spent a significantly greater proportion of time outdoors than grade R children (p<0.001). Overall, educators initiated almost 60% of all activities. However, there were minimal prompts from the teachers in the ECEC settings to increase or decrease physical activity.
Table 4 provides a summary of the multinomial logistic regression results assessing child-level and contextual variables associated with LPA and MVPA in these ECEC settings. Preschool-aged children were more likely to be engaged in LPA (versus sedentary behaviour) if they were in preschool (p=0.008), and if they were transitioning between outdoors and indoors (p=0.004). They were 76% less likely to engage in LPA if they were participating in an activity that was adult-initiated (p<0.001).
In terms of significant factors associated with MVPA (versus sedentary behaviour), children who were classified as overweight/obese were 79% less likely to engage in MVPA compared with normal-weight children (p=0.006), and children were 48% less likely to be engaged in MVPA if they were participating in an adult-initiated activity compared with a child-initiated activity (p<0.001). Being outdoors or in transition (both p<0.001) were both positively associated with MVPA; children were 33 times more likely engage in MVPA if they were outside.
Table 3: Proportion of preschool day spent in selected Observational System for Recording Physical Activity in Children – Preschool Version categories, by setting type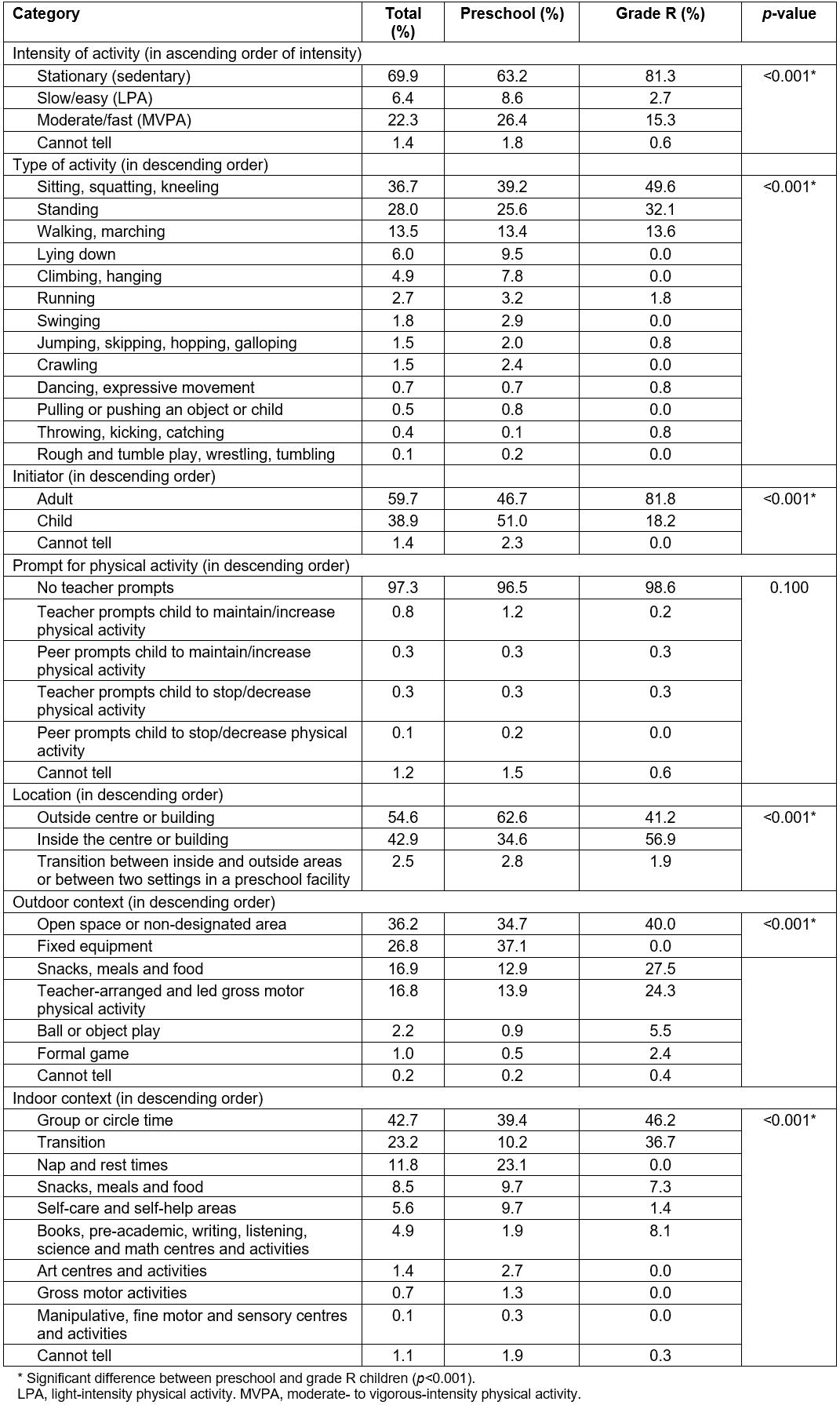
Table 4: Summary of multinomial regression model assessing variables associated with early child education and care physical activity 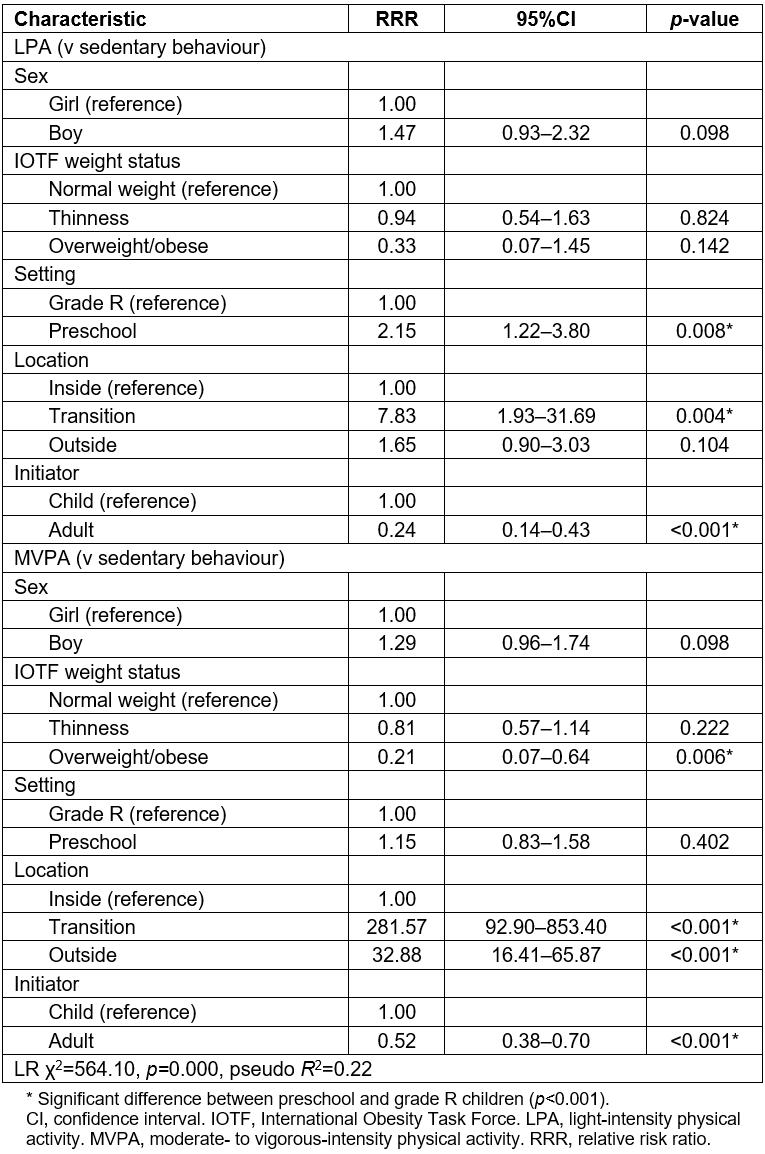
Discussion
This article is the first to describe the physical activity environment of ECEC settings, and to identify child-level and contextual factors associated with physical activity of children within ECEC settings within a low-income, rural South African community. In terms of child-level factors, the fact that overweight/obese children were almost 80% less likely to engage in MVPA compared with their normal-weight peers aligns with research that has identified lower MVPA levels in overweight/obese children in high-income settings30. The relationship between undernutrition and physical activity previously observed in urban South African preschool children was not seen in this rural sample16. This is possibly due to the difference in levels of over- and under-nutrition reported in each sample, particularly in the percentage of children classified as ‘thin’ or underweight (27.3% in this study, 16.3% in the urban study)16. In the present study, no significant associations were found for percentage of time in MVPA and sex, which is contrary to previous research that shows that boys are typically more active than girls in mostly high-income countries5.
In the present study, children at preschools were more likely to engage in LPA in ECEC settings than grade R children. Although a previous review has reported that age is a strong correlate of physical activity within ECEC settings, with older children being more physically active than the younger preschool children5, this finding is more likely because grade R children were in an environment with a greater emphasis on academic learning and thus spent more time indoors sitting at desks or in group activities. In contrast, children in preschools were given more opportunities for free play, spent significantly more time outdoors and had a physical environment more conducive to physical activity (with greater quantities of fixed play equipment and more autonomy to use it) than did the grade R children. Consistent with previous research31, including in South Africa16, children were more likely to engage in MVPA if they were outdoors compared with being indoors. It is worth mentioning that these preschool-aged children in the rural community spent substantially more time outdoors (55%) than reported in urban South African preschool children from low- and high-income settings (7% and 19%, respectively), indicating that, irrespective of proportion of time spent outdoors, preschool-aged children are more likely to be engaged in MVPA when outdoors. It is not surprising that children in these settings were observed to spend the majority of their time in sedentary behaviour, which is comparable to other studies (using the same observational tool) assessing physical activity in urban low- and high-income preschool children in South Africa16, as well as low-income settings in high-income countries, including the USA32.
It is concerning that 5-year-old children in this rural community have already transitioned to formal schooling (grade R within a primary school), where sitting indoors is the predominant activity and they spend less time outdoors. This could possibly be due to the lack of dedicated space to play and the absence of fixed play equipment, which could help to maximise their play time outdoors33. Additionally, the lack of specific physical activity opportunities for the grade R children included in this study is worrying, and presents an opportunity for intervention. According to the national curriculum, grade R children should have physical education as part of Life Orientation, which is allocated 6 hours per week in the curriculum. This is substantially more than the amount of structured physical activity currently allocated in any of the ECEC settings in this study. This may, in part, be due to the lack of training of teachers to intentionally incorporate physical activity into their daily schedule. The limited capacity of teachers to deliver Life Orientation has also been identified in previous studies with teachers in low-income South African settings34,35. This could potentially impact on the capacity of teachers in these ECEC settings to intentionally promote meaningful opportunities for physical activity (low percentage of teacher-led gross motor activities and almost no physical activity prompts by teachers), and a lack of variety of stimulating learning activities within these rural ECEC settings, as suggested by the limited variety of activities in which children engaged.
The higher levels of activity related to child-initiated activity are not unexpected. Similar findings of an inverse relationship of children’s physical activity and staff behaviour have been noted elsewhere26, and the evidence for the role of teachers is in fact mixed5. This suggests that further research should seek to better understand the role of teachers in promoting (or hindering) the physical activity of preschool-aged children in low-income, rural communities in South Africa. It is worth acknowledging that, despite the lack of capacity amongst the teachers in this setting, they do believe in the value of physical activity and associate physical activity in early childhood with better health14.
This study had a number of limitations. The study was conducted in a small number of ECEC settings in one rural community and therefore may not be generalisable to all rural areas of South Africa. Observations were only carried out on one day in each ECEC and thus may not have captured all types of activities undertaken throughout a usual week. The adapted tool used to assess the physical activity environment was not tested for reliability or validity. However, the adapted tool used considered the local context and allowed the researchers to capture information about the setting that has not been captured in previous studies. Additionally, the authors did not assess any physical activity that may take place outside the preschool environment as the focus of this article was to assess preschool-based physical activity. However, 24-hour physical activity has been objectively measured in this setting14, and the high levels of physical activity reported indicate that out-of-preschool activities may contribute to these levels. The authors acknowledge that, in a rural setting, it is possible that much of preschool children’s physical activity would take place outside the preschool hours to do tasks specific to the context. However, this has not been measured in other studies with this age group in South Africa.
Although the OSRAC-P appeared to be a feasible tool for use South African settings, there were multiple outdoor activities built into the OSRAC-P that were not observed at all in these ECEC settings. Thus, it may be necessary for future research in these settings to adapt this tool to suit the environments and contexts being observed. Despite these limitations, the findings of the study have provided insight into a previously under-researched environment. Considering the rate at which rural communities such as those in the Bushbuckridge area are transitioning to an urban health profile36, it is important to understand preschool-aged children’s physical activity within ECEC settings, considering the potential role for these settings in obesity prevention for young children6.
Conclusion
This study reported child-level and contextual factors associated with physical activity in ECEC settings. It is evident that both the physical and social features of ECEC settings are important, and these have implications for how one would promote physical activity in ECEC settings. There are implications for policy, for teachers as well as for the different settings. In terms of policy, the gap between policy (which exists in the primary schools but not in the independent preschools) and implementation needs attention. In this setting, teachers may potentially benefit from being trained and upskilled in physical activity as well as gross motor skill program development and play-based learning. Given the stark differences between preschool type, teachers in the grade R settings and preschool settings should be trained to implement these skills in a way that is appropriate to the environment in which they work. The differences in training and upskilling may be simple. For example, a preschool teacher may benefit more from learning how to use fixed play equipment to improve physical activity than a grade R teacher, who does not have fixed play equipment but has more space. Beyond the ECEC and considering the issues of safety and space allocated for young children to play, it may be beneficial to appeal to local government about promoting safe play for young children by involving older children (as ‘play leaders’), and allocating indoor and/or outdoor space for safe play.
These findings should be viewed within the broader context of early childhood development in ECEC settings, and future research should perhaps look at the relationship between physical activity and other activities in ECEC settings that promote important early childhood development outcomes.
Acknowledgements
The authors thank the preschools and primary schools in Bushbuckridge for allowing them to conduct this research, the parents and caregivers who provided consent, and the Public Engagement Office team within the MRC/Wits Rural Public Health and Health Transitions Research Unit (Agincourt). They are also very grateful to local fieldworker Rose Mnisi, who assisted with the research process.
Funding for this project was provided by the South African National Research Foundation. At the time of this research, SAT was supported by the DST-NRF Centre of Excellence in Human Development at the University of the Witwatersrand, Johannesburg, South Africa; TH was funded by an Australian National Health and Medical Research Council Early Career Fellowship (APP1070571). The MRC/Wits Rural Public Health and Health Transitions Research Unit and Agincourt Health and Socio-Demographic Surveillance System, a node of the South African Population Research Infrastructure Network (SAPRIN), have been supported by the Department of Science and Innovation, the University of the Witwatersrand, and the Medical Research Council, South Africa, and the Wellcome Trust, UK (grants 058893/Z/99/A; 069683/Z/02/Z; 085477/Z/08/Z; 085477/B/08/Z).
References
You might also be interested in:
2020 - Evaluating a centralised cancer support centre in the remote region of Northern Norway
2013 - District specific correlates for hypertension in Kaoma and Kasama rural districts of Zambia