

Introduction
Physical activity can make significant differences in supporting the prevention or treatment of chronic diseases, ensuring that people experience active old age – in other words, enhancing quality of life throughout life1. WHO defines insufficient physical activity as one of the most important health risks. Insufficient physical activity has been found to be linked to a wide range of diseases including cardiovascular system diseases, metabolic diseases, mental health problems, and musculoskeletal system disorders2. Physical activity has been shown to have such benefits as reduced mortality and morbidity, extended life expectancy, and improved mental health. These benefits cover all age groups as well as individuals in special periods such as pregnancy3-6. Despite known health, social, and economic benefits of regular activity, a significant portion of the world population have sedentary lives or fail to engage in regular physical activity7,8.
To ensure higher rates of participation in regular physical activity in society, the desires and tendencies of individuals toward behavior change should be guided using correct approaches. The use of models and theories can provide a systematic methodology and guidance in interventions developed to promote exercise or regular physical activity. A well-defined model can orient effective health promotion programs. The Transtheoretical Model, commonly used to improve the process of health behavior change and achieve the most effective health behavior change, is known to be an extremely effective model for many health behaviors including exercise adaptation1,9-11. This model maintains that people move through various stages, not linearly, but cyclically in exhibiting certain behaviors, and, for this reason, many of them fail to change their lifestyles or retain any change. The model consists of the concepts summarized under four main headings as stages of change, processes of change, decisional balance, and self-efficacy. This model argues that the interventions that are most suitable for the current stage of change of individuals should be used to facilitate change9,10.
The model describes the following stages of change: precontemplation, contemplation, preparation, action, and maintenance12. These stages define change as a gradual, continuous, and dynamic process10. Processes of change are cognitive and behavioral strategies that people use for behavior change. Processes of change provide important guidelines for intervention programs and these processes include some strategies such as consciousness-raising, dramatic relief, self-reevaluation, environmental reevaluation, self-liberation, helping relationships, counterconditioning reinforcement management, stimulus control, and social liberation10,13. Decisional balance focuses on the perceived benefit consequences (pros) and cost consequences (cons) of a behavioral change. It is assumed that an individual can change their behavior when they perceive their positive aspects of behavior. Self-efficacy is the process of trusting your own abilities in the face of some difficulties. It is believed that individuals are more likely to engage in healthy behaviors with greater confidence in their abilities10,14.
The model has been used in connection with many risky health behaviors and behavior change programs involving smokers15, young people16, elderly people12,17, those with cardiovascular disease18, cancer patients13, people with mental disorders19, etc., and it has been sufficiently described for use by every individual.
Predisposing factors that influence health behaviors and can be changed through training are knowledge, attitude, adaptation, and behavior. Cultural disincentives, the distance of healthcare institutions, the small number of diverse healthcare services provided, the small number of healthcare professionals, low education level, socioeconomic status, and other physical deficiencies have an adverse effect on health attitudes of people living in rural areas7,8. Adversities in rural areas such as poor or insufficient healthcare, education, transportation, and other infrastructure pose obstacles to quality of life8,20. The lack of studies investigating the effectiveness of the strategies for reducing sedentary behaviors among adults living in rural areas has been reported as a major shortcoming8. The literature search indicates that the work in this area has been conducted with tiny groups or with groups having specific health problems with a limited number of variables. Moreover, it has been identified that this topic has not been conducted in a rural context. The aim of this study was to investigate the relationship between physical activities of adults living in rural areas and each component of the Transtheoretical Model.
Research questions
Three research questions were posed in this study:
- What are the physical activity levels of the people living in rural areas?
- What are the stages of change, self-efficacy, and decisional balance for exercise levels of the people living in rural areas as well as the predictors of these levels?
- What is the interaction between physical activity levels and the concepts of the Transtheoretical Model in rural areas?
Methods
Research design and settings
This descriptive and relational study was conducted at a rural clinic in Turkey (following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist). The district where the study was conducted is approximately 160 km from the nearest provincial center. Animal husbandry and agriculture are the main livelihoods of the inhabitants. Industrial agricultural applications have recently become widespread in the district. There are kindergartens, primary schools, and secondary schools in the region. Healthcare services are provided in an 80-bed hospital and a family health center. People from the villages nearby come to the district for education and healthcare services.
Participants
The population of the study consisted of the individuals living in this district and the villages that are administratively attached to it. The study group comprised the individuals who visited health clinics for themselves or for their relatives for any reason, and those with physical and mental abilities were not included. Of the individuals who took part in the study, 63% lived in villages and 57% in the district. Based on an effect size of 0.15, a statistical power of 95%, and a significance level of 0.05, the minimum sample size was found to be 315 for the design of the study21. The sampling sufficiency was evaluated for the analysis used in the study. For each independent variable, 20–60 data were needed for logistic regression, 10–20 data for multiple regression22, and at least 300 data for path analysis23. The sample size of the study was found to be sufficient for analysis.
Instruments
The data were collected using a survey form inquiring about the sociodemographic characteristics of the individuals, the Stages of Change for Exercise Short Form, the Self-efficacy for Exercise Scale, the Decisional Balance for Exercise Scale and the International Physical Activity Questionnaire. The Stages of Change for Exercise Short Form, the Self-efficacy for Exercise Scale, and the Decisional Balance for Exercise Scale are the measurement tools that assess the Transtheoretical Model. Although the Processes of Change for Exercise Short Form is part of the Transtheoretical Model, it was not used in this study due to the problems the individuals living in rural areas encountered in understanding it. Other scales had high Cronbach’s alpha levels in the study group and were included as the data collection tools in the study.
Survey form
The survey form included questions about age, gender, marital status, education level, income level, and chronic disease status of participants.
Stages of Change for Exercise Short Form
Developed by Marcus et al24, the Stages of Change for Exercise Short Form consists of five questions. The form assesses the current exercise status of the individual and his/her future intentions about exercising. The question responses reveal the stage of change of a respondent. Form scoring is as follows: respondents who do not exercise and do not intend to in the next 6 months are in the precontemplation stage; those who do not exercise but intend to in the next 6 months are in the contemplation stage; those who do not exercise but intend to in the next 30 days are in the preparation stage; those who have been exercising for less than 6 months are in the action stage; and those who have been exercising for more than 6 months are in the maintenance stage. In the internal consistency analysis, Cronbach’s alpha coefficient of the scale was found to be 0.9524. In the present study, Cronbach’s alpha was 0.91. As in the study of Romain and Abdel-Baki (2017)19, this study considered the first three stages as the pre-action stage and the last two stages as the pro-action stage.
Self-Efficacy for Exercise Scale
The scale, developed by Marcus et al24 assesses self-efficacy of individuals in controlling their behaviors for exercising in different situations (eg in various weather conditions). The highest and lowest scores from this five-point Likert-type scale consisting of six items are 30 and 6, respectively. In the assessment of the scale, higher item score means indicate higher self-efficacy. In the internal consistency analysis, Cronbach’s alpha coefficient of the scale was found to be 0.9024,25. In the present study, Cronbach’s alpha was 0.84.
Decisional Balance for Exercise Scale
This scale was developed by Marcus et al24 to evaluate individuals’ perceived benefits (pros) and costs (cons) associated with exercise behavior. The scale assesses an individual’s subjective perceptions about the positive and negative consequences of exercising that influence their exercise behavior. Scores are obtained for the pros and cons of subdimensions of the scale, and the total score of the scale is calculated by subtracting the total pros scores from the total cons scores. In the internal consistency analysis, Cronbach’s alpha coefficient of the scale was found to be 0.8624,25. The pros and cons scores of the scale were employed as distinct variables for better assessment of the relationship in the analysis.
International Physical Activity Questionnaire
The International Physical Activity Questionnaire was developed by WHO and the US Centers for Disease Control and Prevention, and its validity and reliability test for Turkish was conducted by Saglam et al26. It presents information on the time individuals spend on light, medium, and vigorous activities and in sitting. For evaluation, each activity should be performed for at least 10 minutes at a time. The metabolic equivalent of task (MET) values for each activity category (walking = 3.3, moderate activity = 4, vigorous activity = 8) are multiplied by day and minutes to obtain the MET-minutes/week scores. Based on their MET-min/week scores, individuals are classified into low activity (<600 MET-min/week), moderate activity (600–3000 MET-min/week), or vigorous activity (>3000 MET-min/week) categories, and the total energy spent by the individual in the activity category is calculated26. In this study, the individuals were classified according to the exercise difficulty level, and total MET-min/week was calculated in the analysis.
Statistical analyses
The Statistical Package for the Social Sciences v22 (IBM; http://www.spss.com) was used for analyzing the data. The obtained data were shown as number, percentage, and mean. Logistic regression analysis was conducted to assess the risk factors of the pre-action stage. Multiple regression analysis was used to find the predictors of the self-efficacy level, perceptions of the pros and cons of exercise, and total MET values. Categorical data were coded as 0 and 1 for the logistic and multiple regression analysis. Age, self-efficacy for exercise score, decisional balance for exercise score, and total MET value are continuous variables. Gender (female: 1; male: 0), education level (primary school: 1; secondary school and higher: 0), marital status (married: 1; single: 0), income perception (bad and medium: 1; good: 0), chronic disease (yes: 1; no: 0), and stage of change level (pre-action: 1; post-action: 0) were recoded. Path analysis was conducted to illustrate how the Transtheoretical Model interacted in rural areas. The physical activity level (MET value) was taken as the result variable. Various models were tested to determine how the Stages of Change for Exercise Short Form, the Self-efficacy for Exercise Scale, and the Decisional Balance Scale for Exercise influenced this result. Fit indices were evaluated to find the best model (χ²/standard deviation, goodness of fit index (GFI), adjusted goodness of fit index (AGFI), comparative fit index (CFI), standardized root mean square residual (SRMSR), and root mean square error of approximation (RMSEA)). Significance was evaluated to be p<0.05.
Ethics approval
This study was approved by the Non-Interventional Clinical Research Ethics Board (2018/131) of Selcuk University. Written approval was obtained from the directorate of the hospital, and patients gave written consent prior to the research.
Results
The average age of the participants was 43.79±14.49. Of the participants, 67.9% were females, 70.9% were married, 50.6% were primary school graduates, and 54.2% had paid jobs. More than a quarter of the individuals (26.1%) perceived their income level as good, while 36.1% of the participants had chronic diseases. Regarding the Stages of Change for Exercise Short Form, 42.4% of the participants were in the precontemplation stage, and 23.3% expressed that they would start exercising in 6 months while the rate of those who intended to start exercising was 7.9%. The ratio of the participants who had been exercising for less than 6 months was 11.2%, whereas 15.2% had been exercising for more than 6 months. The mean self-efficacy for exercise score was 12.9±6.5, and the mean scores of cons subdimension and pros subdimension of decisional balance for exercise were, respectively, 1.2±4.1 and 16.5±5.7. The decisional balance for exercise tilted toward the cons for 32.7% of participants and the pros for 69.7% of participants. According to the International Physical Activity Questionnaire, 59.1% of the individuals living in rural areas were inactive, and 29.1% engaged in moderate exercise and 11.8% in vigorous exercise. The total average of the MET value was 1055.0±1507.0.
Higher self-efficacy scores (CL:0.904 GA:0.859–0.951) and longer MET duration (CL: 0.998 GA: 0.997–0.999) serve as a protective factor in the pre-action stage of the exercise behavior (Table 1). The predictors of the Decisional Balance for Exercise Scale were education status (β=0.191) and marital status (β=0.121). Low education level and being married increased the cons score (R2=0.095). For the pros subdimension, increasing age (β=–0.222) reduced the pros score whereas an increase in income level (β=0.134) and self-efficacy score (β=0.428) increased the pros score (R2=0.309) (Table 2). Education level at or below primary school (β=–0.158), lack of intention to start exercising (β=-0.166) and increased cons scores of exercise scores (β=–0.092) were the variables that negatively affected self-efficacy. In contrast, increased pros of exercise scores (β=0.385) and increased MET level (β=0.197) were the variables that positively affected self-efficacy. The coefficient of determination was 38% (Table 3). The predictors of the mean MET value of the participants were gender, being in the pre-action stage, and the self-efficacy score. Being a woman (β=–0.120) and being in the pre-action stage (β=–0.329) decreased the MET score whereas the increased self-efficacy (β=0.233) increased the MET score. These two variables explained 27% of the MET score (Table 4).
Path analysis was used to assess how the scales that evaluate the exercise behavior from different perspectives influence each other conceptually. Different models were evaluated, and the model given in Figure 1 was created based on the best-fit indices. The χ2/degrees of freedom value of the model was found to be 1.173, GFI: 0.99, AGFI: 0.97; CFI: 0.99; RMSEA: 0.023 and SRMS: 0.02. In previous models, there was no relationship between the cons subdimension and pros subdimension of decisional balance for exercise and physical activity behavior (MET score). Similarly, there was no relationship between the pros subdimension of decisional balance for exercise and stage of change for exercise. The latest model was created according to this information.
According to this model, the perceived benefits of exercise (pros) had a positive effect on the perceived self-efficacy (β=0.476), and the perceived costs of exercise (cons) (β=–0.149) had a negative impact on self-efficacy and stage of change for exercise whereas increased self-efficacy (β=–0.108) positively affected stage of change for exercise (β=0.362). In addition, both self-efficacy (β=0.255) and stage of change for exercise (β=0.367) influenced the physical activity behavior (MET score). The standardized total and direct effect values of the variables are given in Table 4. Based on these values, in the emergence of exercise behavior in rural areas, the perception of cons of exercise of the participants directly affected self-efficacy and stage of change for exercise and contributed to the total effect on the MET score. The perceived pros of exercise had a direct effect on self-efficacy and contributed to the total effect on stage of change for exercise and the MET score. The perceived self-efficacy had both direct and total effect on the MET score as well as on stage of change for exercise. Stage of change for exercise was the variable that had a significant effect on the MET score.
Table 1: Risk factors for pre-action stage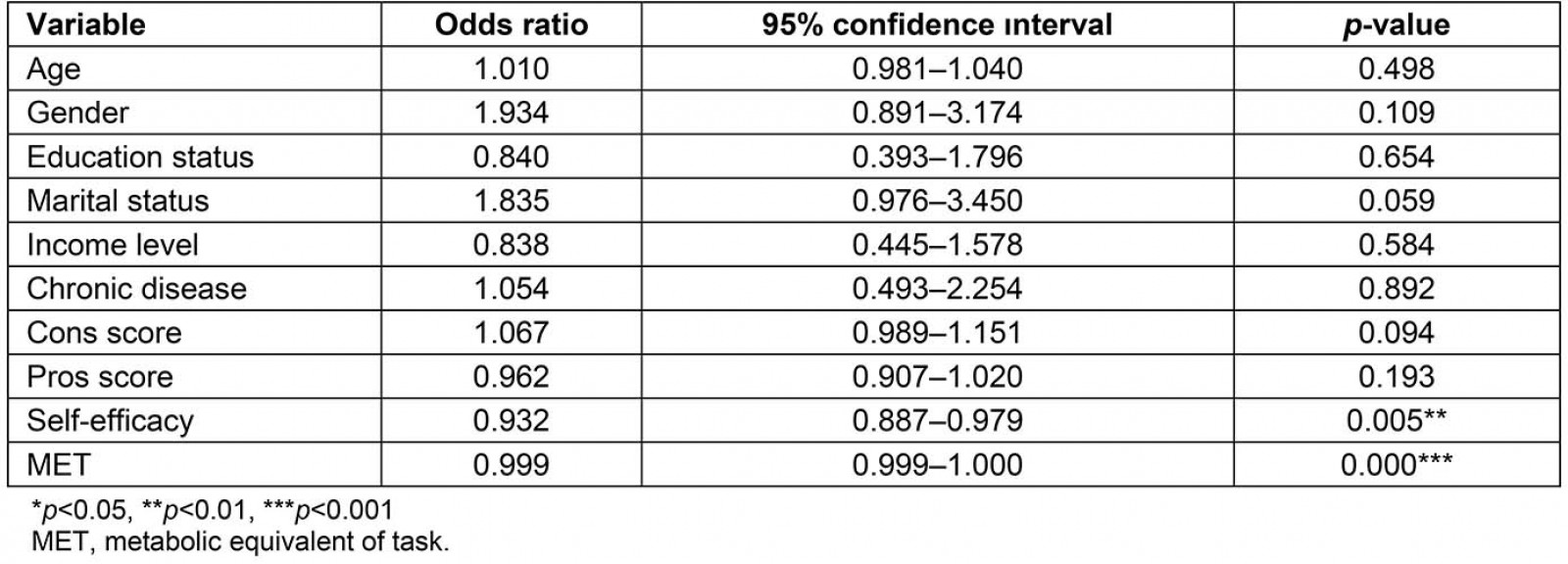
Table 2: Determinants of decisional balance scale for exercise (cons and pros subdimensions)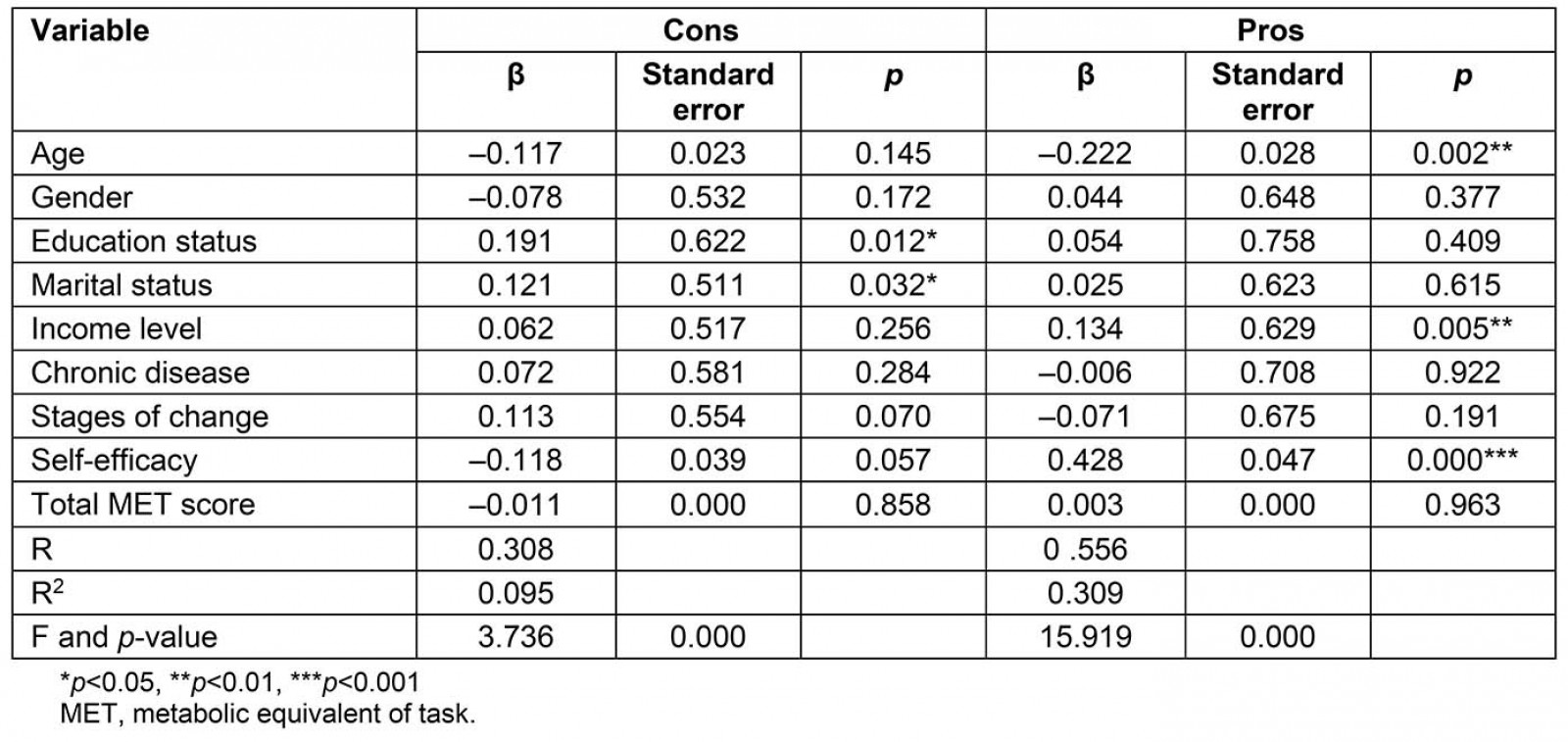
Table 3: Determinants of self-efficacy level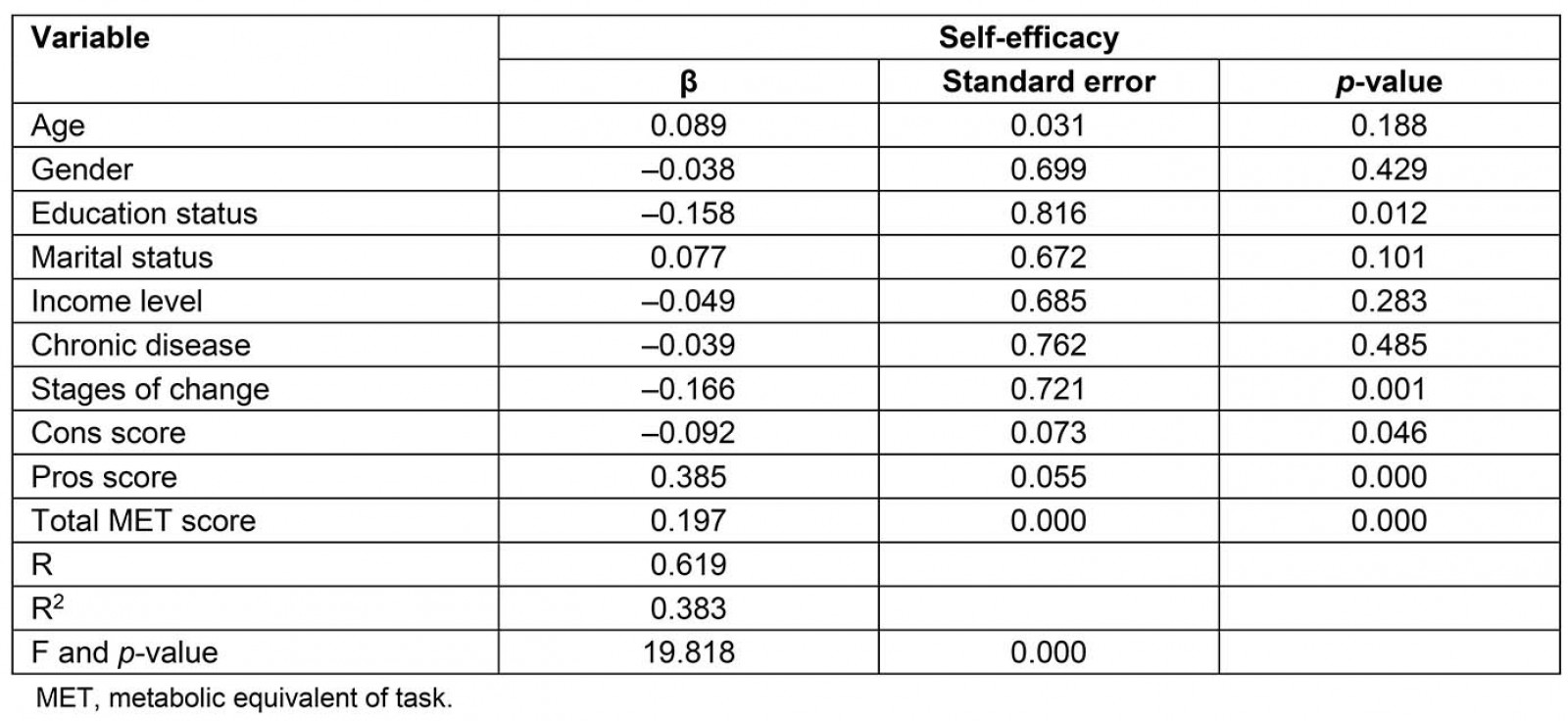
Table 4: Determinants of MET level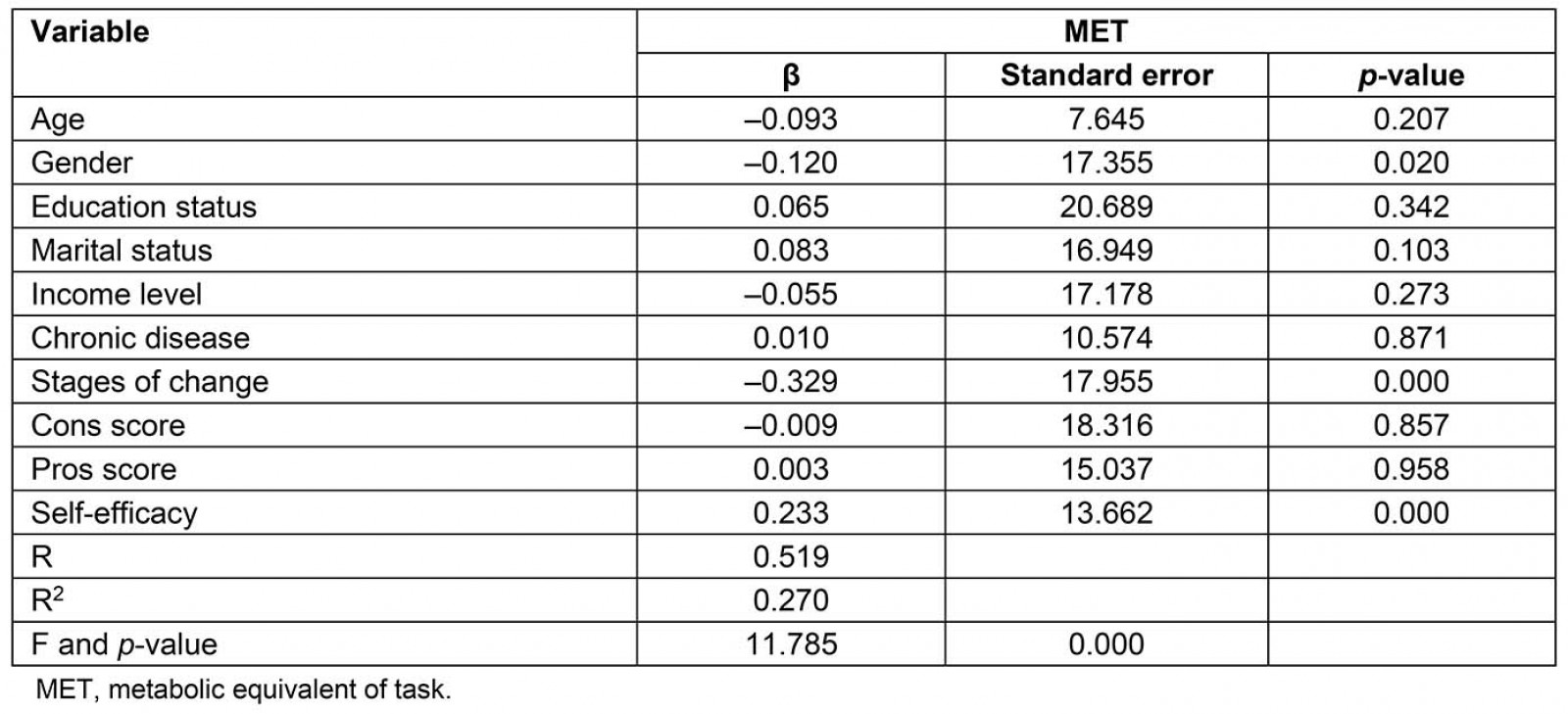
Table 5: Interaction between physical activity levels and concepts of the Transtheoretical Model in rural areas with path analysis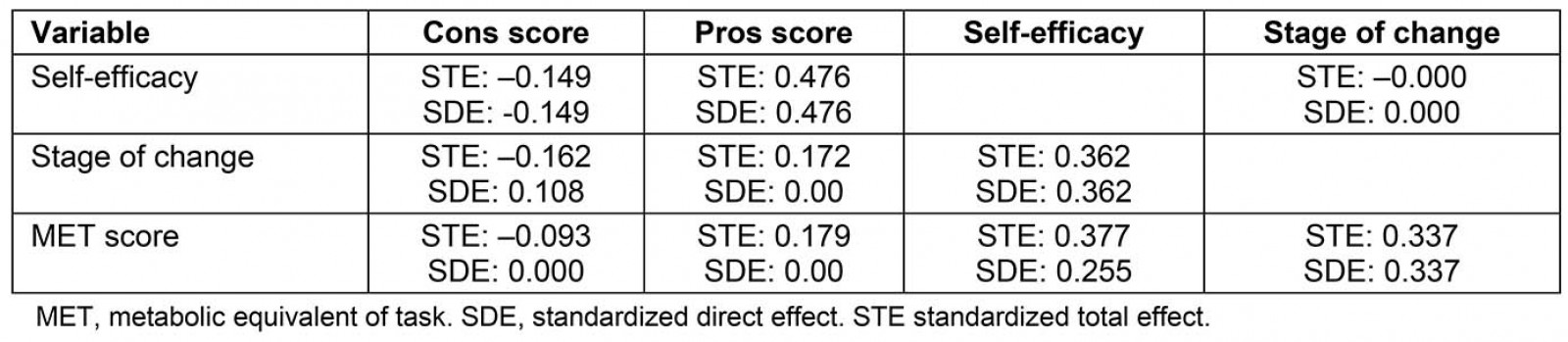
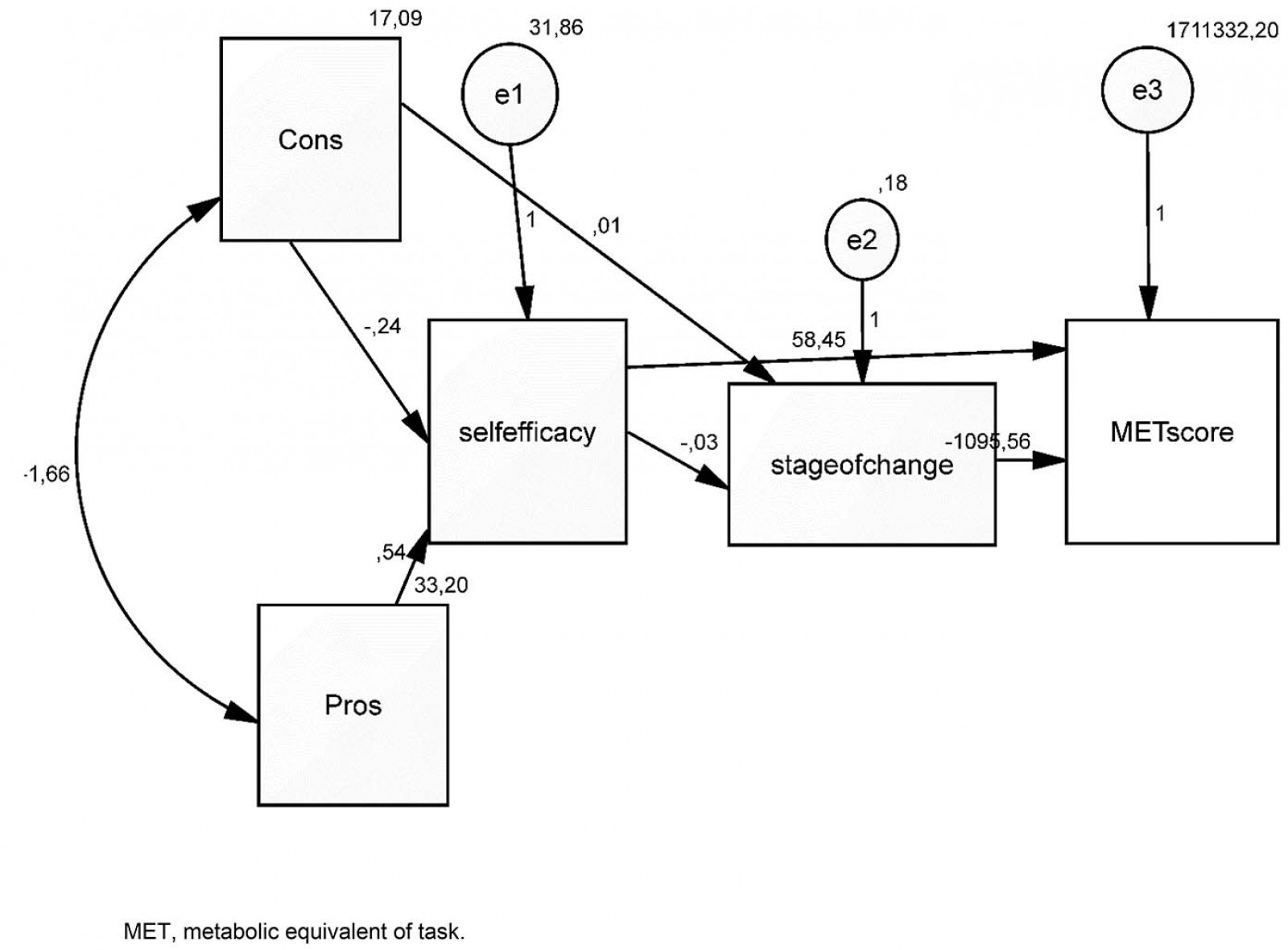 Figure 1: Interaction between physical activity levels and the concepts of the Transtheoretical Model with path analysis.
Figure 1: Interaction between physical activity levels and the concepts of the Transtheoretical Model with path analysis.
Discussion
In the study, it was found that more than half of the participants living in rural areas were inactive, and the rate of those who had been exercising for more than 6 months was low. The WHO recommends moderate-intensity aerobic physical activity for at least 150 minutes per week and vigorous-intensity physical activity for at least 75 minutes per week for adults27. The exercise behavior of the study group was far less than the recommended amount. The physical activity levels are influenced by the places where individuals live28. In a study conducted in a rural area, 10.1% of the participants were reported to engage in physical activity for at least 150 minutes per week7. On the other hand, a study with individuals aged between 35 and 74 years in China found 78.1% of the residents of the rural area to be physically active. These differences suggest that the characteristics of rural communities may change among countries, and rural occupational diversities may explain the difference. A meta-analysis that focused on rural areas reported widespread sedentary lifestyles among adults living in rural areas, stressing the lack of effective strategies for reducing sedentary lifestyles8, whereas another meta-analysis argued that interventions significantly improved the physical activity behavior29. The results of the present study suggest that the rural population should be considered as a high-risk group due to insufficient physical activity.
The effect of cultural differences and rural or urban lifestyles on health behaviors has been reported in the literature2,24. In addition, given that physical activity interventions in rural areas are highly ineffective8, the use of models based on culture and individual characteristics in investigating exercise behavior in rural areas are gaining prominence. In this study, the exercise behavior was examined based on the Transtheoretical Model due to the convenience it provides in understanding and explaining health behaviors.
The stages of change in this model define the interest and motivation of individuals concerning behavior change10. A large portion of the participants were in the precontemplation stage about starting exercise. Therefore, their enthusiasm and motivation in exercise were negative. The study found no relationship between the socioeconomic characteristics of the participants and the stage of change and identified increased self-efficacy, and MET levels as a protective factor for the pre-action stage. However, the cause and effect relationships among these three concepts should be examined using path analysis, and according to the path analysis conducted, the perception of self-efficacy had a positive effect on the stage of change, and the positive change in stage of change led to increased MET levels. A study reported that self-efficacy increased further when individuals moved from the preparation stage to the action stage19. Kirk et al (2010) reported a regular increase in self-efficacy scores from the precontemplation stage to the maintenance stage while finding that the 7-day physical activity level was the lowest in the precontemplation stage and the highest in the action stage12.
In the present study, the decisional balance for exercise pros score of the participants was higher, but the mean scores of both cons subdimension and pros sub-dimension were low. The decisional balance for exercise tilted toward the cons in 32.7% and the pros in 69.7%. Although these results suggest that the participants might have positive perceptions about the exercise behavior, the low scores from the pros and cons subdimensions imply that they had low exercise awareness, and they had low chances of deciding to change24. Low education level and being married increased the cons score while income level and self-efficacy score increased the pros score. Therefore, these individuals need to be strengthened through health training, exercise opportunities should be created for married individuals, and their self-efficacy perceptions should be improved. The relationships between education and income levels and health behaviors are well defined under the Ottawa Charter for Health Promotion, and these variables are considered as prerequisites of health behaviors30. Also, based on path analysis, it was found that perceptions of both pros and cons of exercise had a direct or indirect effect on self-efficacy for exercise, stage of change for exercise, and physical activity level.
In this study, the self-efficacy for exercise levels of the participants was low. Improvement of self-efficacy, which has been put forward as the main concept in many theories about health behaviors, is an effective way to increase physical activity31. In the present study, the self-efficacy levels of the participants were affected negatively by low educational level and lack of intention to start exercising, and positively by the increased benefit of exercise scores and the MET levels. Self-efficacy is important to overcome barriers to physical activity. It was demonstrated that self-efficacy was a predictor of the stage of change for exercise and effective in bringing up the behavioral processes of change16. Based on path analysis, it was found that raising awareness of individuals about the benefits of exercise had a significant effect on self-efficacy. Positive change in the perceptions of self-efficacy increased the stage of change for exercise and the physical activity level.
Limitations
The present study is limited to the answers received from people aged 18–65 years living in a rural area within the borders of some village in Konya city. Data obtained are based on personal feedback of participants, hence all answers reflect truth only to the extent of the interests and focus of participants. Additionally, in this observational study, there is no comparison group. The Processes of Change for Exercise Scale, which is part of the Transtheoretical Model, was not used in this study due to the problems the individuals living in rural areas encountered in understanding it. This scale could offer contributions to improve exercise behavior. To increase the usability of the model in rural areas, it is important to modify the Processes of Change for Exercise Scale for rural areas and to evaluate its validity and reliability. Although this study is a relational study, the results of the regression and path analysis used in this study would guide the interventions to be developed to make exercise more widespread.
Implications
Healthy aging is a significant health goal for countries, and the importance of physical activity in this process is well known. However, the rate of inactive people in societies is alarming, and the prevalence of inactivity varies widely among countries. Therefore, it seems necessary for each culture to plan an intervention32. The Transtheoretical Model is known to be an advantageous model for many health behaviors, including exercise adaptation. This study enables the assessment of exercise behaviors of people living in rural areas with the Transtheoretical Model.
Conclusion
The findings of this study revealed that individuals living in rural areas had insufficient physical activity levels. People living in rural areas should be considered as a high-risk group in terms of exercise behavior. In terms of perceptions that affect the decision to start exercising, awareness levels were low, and people had insufficient self-efficacy levels and negative attitudes in relation to stage of change for exercise. Age, education, marital status, and income are sociodemographic characteristics that are determinants for the concepts of the Transtheoretical Model. The Transtheoretical Model is believed to be a strategic approach to developing exercise behavior in rural areas. Path analysis offers important points about the sequence of the content of interventions. Interventions in rural areas should include practices regarding perceptions of benefits and costs of exercise. Interventions designed to increase individual self-efficacy should be preferred in the second phase of inventions. Creating motivation for individuals for the stage of change for exercise would be meaningful only after ensuring a satisfactory level of self-efficacy. The perceived self-efficacy and stage of change for exercise were the most important variables that had a significant effect on the MET score. As a result of the interventions that include these phases, it may be possible to increase the physical activity levels of individuals. Also, the prerequisites of health promotion, such as enhancing education, income, and opportunities, will contribute to the scale-up of exercise.