
Introduction
The annual global burden of snakebite is 81 000–138 000 lives, and many more permanent limb injuries and amputations1,2. Annually, sub-Saharan Africa experiences a significant proportion of the global burden from snakebite, with approximately 300 000 envenoming bites and 10% of these bites resulting in death or permanent disability3. In June 2017, the WHO designated snakebite envenoming a neglected tropical disease4. Like many neglected tropical diseases, snakebite envenoming is largely a disease of poverty5. Rural populations, farm workers, herders, children, and communities with limited access to education and health care, are among the highest risk groups for this neglected issue2,5.
Snakebite envenoming is a medical emergency that requires rapid diagnosis and appropriate antivenom treatment to neutralize the snake venom6. Any delay to receiving antivenom treatment could potentially mean loss of life or limb6. Children are especially vulnerable to snakebite envenoming, and they experience higher risk of causal morbidity and mortality6. The sensitivity of the victim’s response to the venom varies by individual case, and children typically experience the effects more quickly than adults due to smaller body mass6.
The Kingdom of Eswatini, formerly known as Swaziland, is a sovereign state in Southern Africa that includes 1.3 million people, of which 79% live in rural areas7. Snakebite envenoming is often neglected as a public health issue in Eswatini due to an HIV prevalence rate of 26%, the world’s highest tuberculosis incidence rate and limited public health resources7. However, 62 snake species reside in the region, of which, seven species, known as the ‘seven deadly sins,’ are considered to be extremely dangerous8. Of these, the Mozambique spitting cobra (Naja mossambica), puff adder (Bitis arietans), black mamba (Dendroaspis polylepis), snouted cobra (Naja annulifera) and the rinkhals or ring-necked spitting cobra (Hemachatus haemachatus) are responsible for the majority of life-threatening bites, over 200 reported annual deaths, and many more long-term disabilities in the region8,9.
Similarly to many sub-Saharan African countries, Eswatini has a shortage and unequal distribution of effective antivenom and a lack of adequate medical facilities to treat snakebite in the rural communities most vulnerable to snakebite10. The availability of antivenom is limited due to a collapse of commercial production in Africa11. Besides distance barriers to proper medical treatment, rural communities experience financial, language and cultural barriers, which often deter snakebite victims from receiving antivenom treatment5,12.
The Eswatini Antivenom Foundation strives to reduce the burden of snakebite envenoming by supplying free antivenom and organizing community engagement programs to educate communities about snakes13. The foundation is also responsible for the majority of snake education programs around the country, and it plays a critical role in mitigating the burden of snakebite envenoming in the region13. Community engagement programs are valuable methods for tackling health inequalities and providing a voice to vulnerable populations that experience the largest health burden from those inequalities12. An urgent need remains for appropriate community engagement programs to raise awareness about prevention and treatment for this neglected disease – specifically, educational tools targeted to children in Eswatini, given that this population is particularly vulnerable to snakebite6.
Musical interventions have been shown to be an effective teaching tool in community engagement programs that focus on public health issues14,15. In South Africa, in an effort to appropriately educate the public about HIV, entertainment education or ‘edutainment’ became a popular teaching tool14. Jiving with Science was an example of edutainment that developed and distributed edutainment CDs over two years14. The aim of the intervention was to deliver evidence-based health promotion messages about HIV/AIDS to everyday spaces14. Edutainment was effective for HIV awareness because audiences were engaged and identified themselves in the messages conveyed14. In The Gambia, music was found to be an effective, culture-centered approach to disseminate sensitive public health topics and may promote trust between health professionals and target communities16. Using existing community traditions such as music may offer a culturally appropriate tool to enhancing community snakebite awareness programs in an engaging, affordable, sustainable and accessible form14.
The musical intervention in this study, Iculo ngenyoka, is a form of edutainment dubbed a NuRhyme to describe modern-day nursery rhymes that address a health threat to children17. Eoin Harrington created Iculo ngenyoka or 'Snake song' and the innovative concept of Nurhymes with the goal of leveraging music in the form of nursery rhymes to disseminate public health information to children around the world. Iculo ngenyoka was written and sung for communities in Eswatini to inform children about the dangers of snakebite in the region. However, research has not explored or described the acceptability and potential use of a musical intervention, such as a NuRhyme, as an educational tool for snakebite awareness and prevention.
This was an exploratory study to discover if the use of the Iculo ngenyoka song was a feasible and acceptable tool to raise awareness in rural communities in Eswatini, particularly among children, about snakebite. The study explored the attitudes and perceptions among rural families and students about the musical intervention in Eswatini to understand if it was an acceptable teaching tool and whether it had a potential use in snake awareness community engagement programs in the region.
Methods
Location and study subjects
Qualitative data were collected in the Lubombo region of Eswatini. Participants were selected from four separate communities within the Lubombo region: Simunye, Nyetane (St Augustine Primary School), Mabuda Farm (Siteki) and Makhewu (Siteki) (Fig1). The Lubombo region was chosen because local populations are highly vulnerable to the burden of snakebite and few medical facilities are equipped to treat snakebite envenoming.
The participants were residents of the Lubombo region and spoke either siSwati or English languages. Three types of participant were recruited:
- parents/guardians: individuals considered to be the elders in their homesteads, aged 18–64 years
- children: individuals aged 7–17 years
- key informant: expert and director of community engagement programs and snakebite treatment education in Eswatini.
A combination of convenience, snowball and purposive sampling techniques were used to identify and recruit a sample of participants with the assistance of onsite mentors and two local interpreters in all four locations.
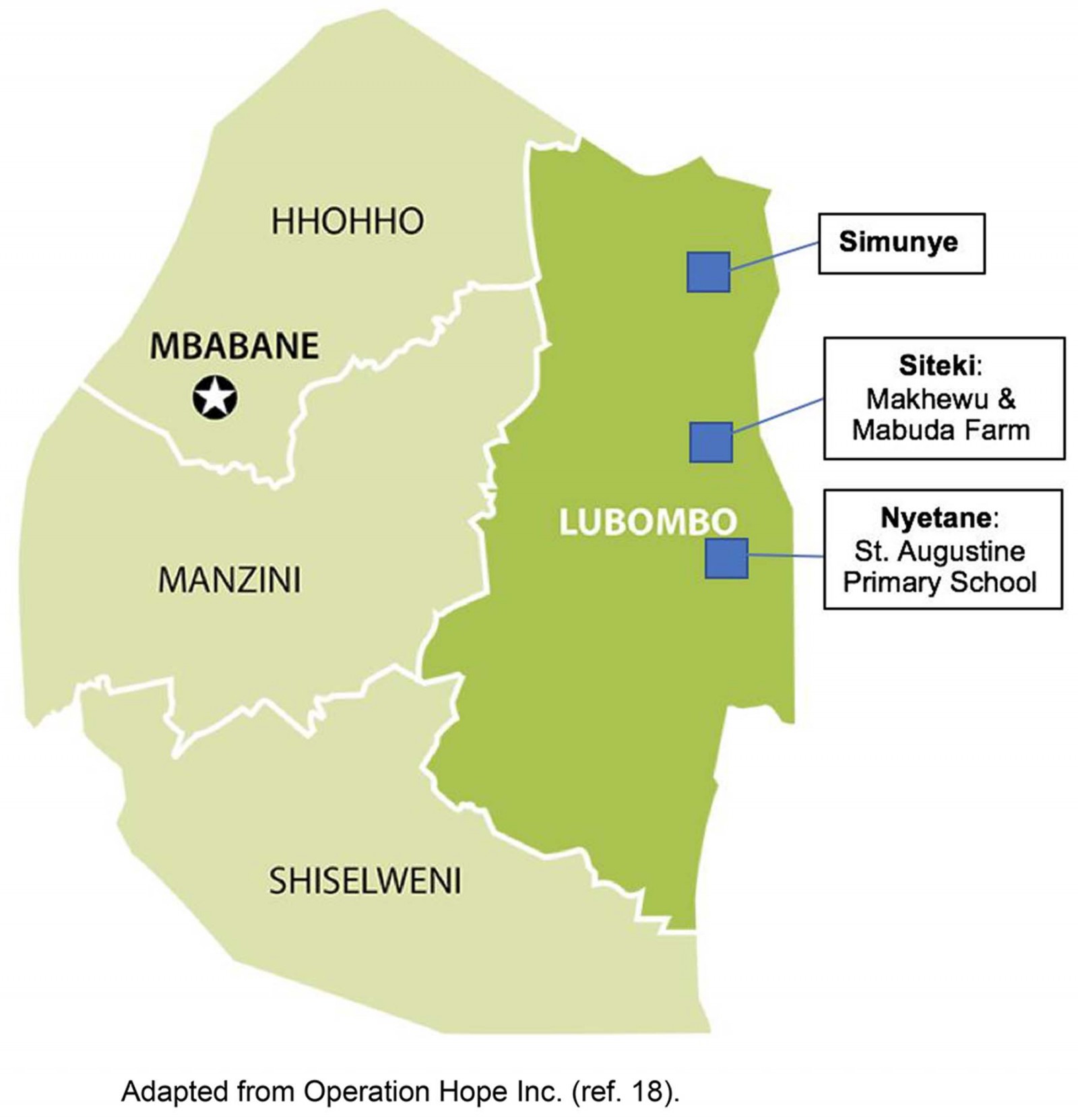 Figure 1: Participants were selected from four communities within the Lubombo region of Eswatini: Simunye, Nyetane, Mabuda Farm and Makhewu18.
Figure 1: Participants were selected from four communities within the Lubombo region of Eswatini: Simunye, Nyetane, Mabuda Farm and Makhewu18.
Data collection
The parent/guardian participants and/or the children’s legal guardians were asked to sign an informed consent form to participate in the study. It was also necessary for the children participants to provide verbal consent to participate. All participants received copies of the consent forms in siSwati. After consent was obtained from the participants, the musical intervention was played, followed by a semi-structured qualitative interview.
Participants received compensation for their time and energy in the study. The parent/guardian participants were compensated household supplies to the value of $5, such as kitchen towels, bag of oranges, soap, corn meal and rice. The children participants were compensated school supplies to the value of $5, such as pencil bags, stickers, pens, pencils, erasers, rulers, colored pencils and school notebooks.
Iculo ngenyoka musical intervention
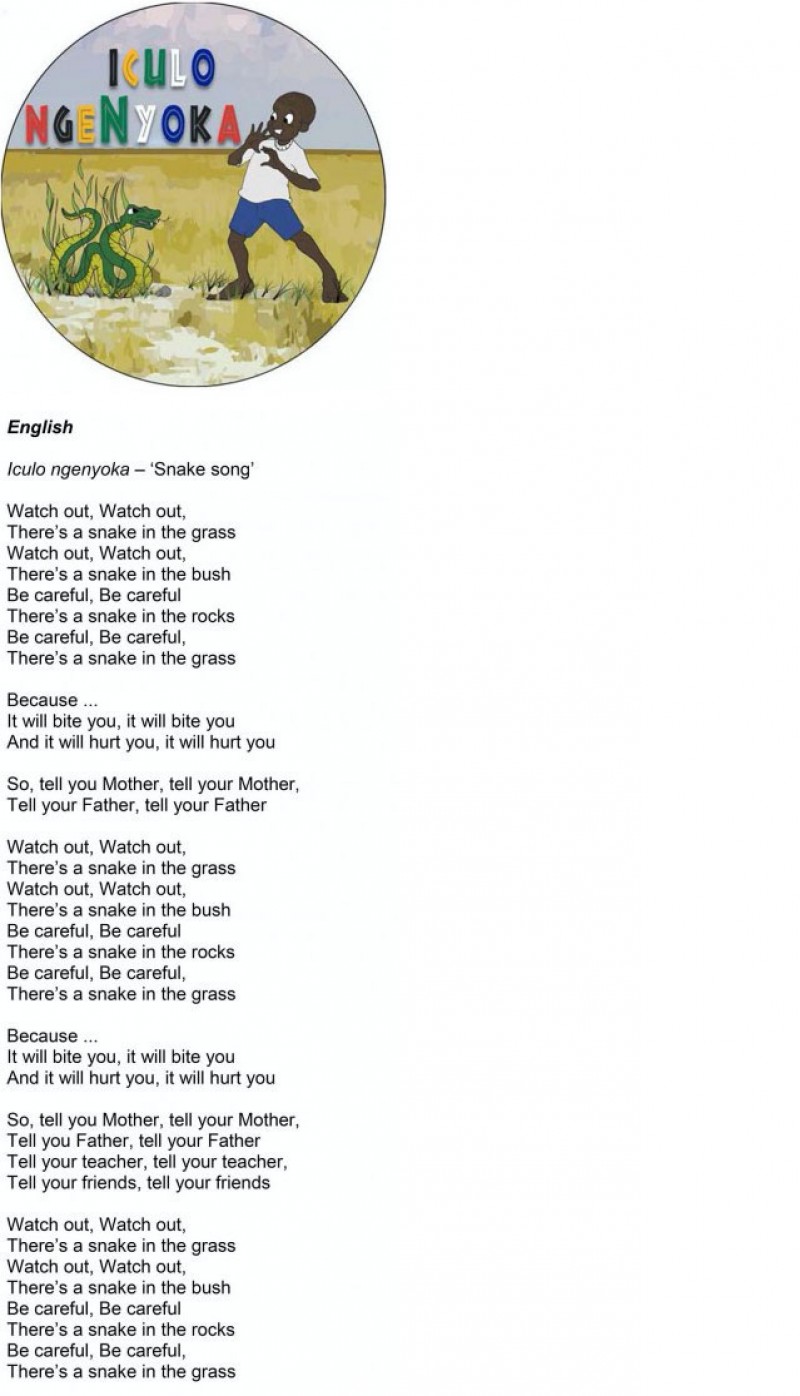
The musical intervention, Iculo ngenyoka, was written and composed by Eoin Harrington and translated and performed in Zulu by the founder of the South African Zulu Spear Band, Gideon Bhendile, who also provided insight regarding cultural relevance of the song. Zulu and siSwati are derived from the African languages with minor variations in dialect and tones; however, siSwati has acquired written status and is the official language in Eswatini19. Speakers of siSwati understand Zulu and vice-versa19. The song duration was 1 minute and 43 seconds and followed the nursery rhyme structure of (1) what to look out for, (2) why you should care and (3) what you should do. The song’s message was (1) snakes hide under rocks, in the grass or in bushes, (2) snakes can bite and hurt you and (3) tell your father, mother, teacher and friends if you see a snake or are bitten by one. The lyrics and an audio link are attached in Appendix I.
The song was played through a portable speaker and participants could request to listen to the song as many times as they wanted to. The song was also shared with the elder participants that had a cell phone, and the head teacher at St Augustine Primary School.
Qualitative interviews
Following the song, semi-structured interviews of 20–60 minutes each were conducted with the assistance of an interpreter. At Mabuda Farm and St Augustine Primary School, small focus group interviews (2–4 participants) were conducted. In the Makhewu community, based on the availability of potential participants at the homesteads, either one-on-one or small focus group interviews (2–4 participants) were conducted. In Simunye, a one-on-one interview was conducted with the key informant.
Semi-structured interview guides were developed for all study groups. Overall, the guides were used to explore participant attitudes and perceptions about the musical intervention and the burden of snakebite in their communities. During the interviews, participants were asked to describe their understanding of the song, previous snake experiences/stories, their attitudes about snakes, their attitudes and perceptions of the song as a tool to raise awareness about snakes, and if they would recommend the song to someone they know. Lines of questioning differed slightly across the three types of study participant. Parents/guardians were asked specific questions regarding their attitudes and perceptions of the song being taught to their children and played in their homestead. Parents/guardians were likely to have had previous encounters with snakes in their community, so questions were tailored to understand their health-seeking behavior and information they taught their children about snakebite prevention and treatment. Children were asked specific questions regarding their attitudes and perceptions of the song being taught at their school and to their friends. The key informant was a snake expert, who was asked questions pertaining to the severity of snakebite envenoming in the country, strategies to mitigate the burden and if the song is an appropriate tool to educate communities about the dangers of snakes in the country.
Two local interpreters (one male and one female) assisted author LTE during the data collection process when necessary. To improve participant comfort, a male interpreter accompanied the male interviewees, and the female interpreter accompanied the female interviewees.
The interviews were audio-recorded with each participant’s consent. Interviews were conducted in a time and space that was comfortable to the participants. Notes were taken before, during and after the interviews. For the siSwati interviews, LTE transcribed the English dialog, verbatim, between him and the interpreter. The key informant interview was transcribed verbatim as well. The audio-recordings were stored in a safe place until they were transcribed onto a password-protected, encrypted computer. After the interviews were transcribed, the audio-recordings were erased.
Analysis
A framework analysis approach was used to analyze the interviews20. A codebook was drafted after LTE read through the interview guides and each transcript, and consequently revised with suggestions from co-authors. After reading through each transcript, coding topics were established that could be applied across all interviews. The transcripts were entered into Dedoose v8.0.42 (http://www.dedoose.com), a program designed to organize qualitative data. The coded transcripts were used to formulate a framework analysis table, which was organized with a coded summary for each of the participants20. This method of organizing qualitative data facilitates the identification of themes across the participants. Based on the aims for this study and a framework analysis table, main themes and subthemes emerged, which are described in the results. The student researcher transcribed the interviews and preliminary analysis, and the codebook and transcripts were shared with the research team to check the interpretation of the data.
Ethics approval
All procedures were reviewed and approved by the Institutional Review Board at the University of California, San Francisco (IRB approval number 18-24644). Local permission to conduct the study was granted by school authorities and/or village leaders in the respective communities.
Results
A total of 22 qualitative semi-structured interviews were conducted between May and June 2018. The interviews occurred in four communities in the Lubombo region of Eswatini. All participants (n=56) were local residents; the age of the youngest participant was 7 years and the age of the oldest participant was 64 years (Table 1).
The data were organized into three domains: (1) knowledge, attitudes and local practices, (2) current education tools about snakes and (3) attitudes and acceptability of the Iculo ngenyoka musical intervention. Within these domains, five main themes and eight subthemes were identified (Table 2).
Table 1: Characteristics of interviewees (n=56) in the Lubombo region, Eswatini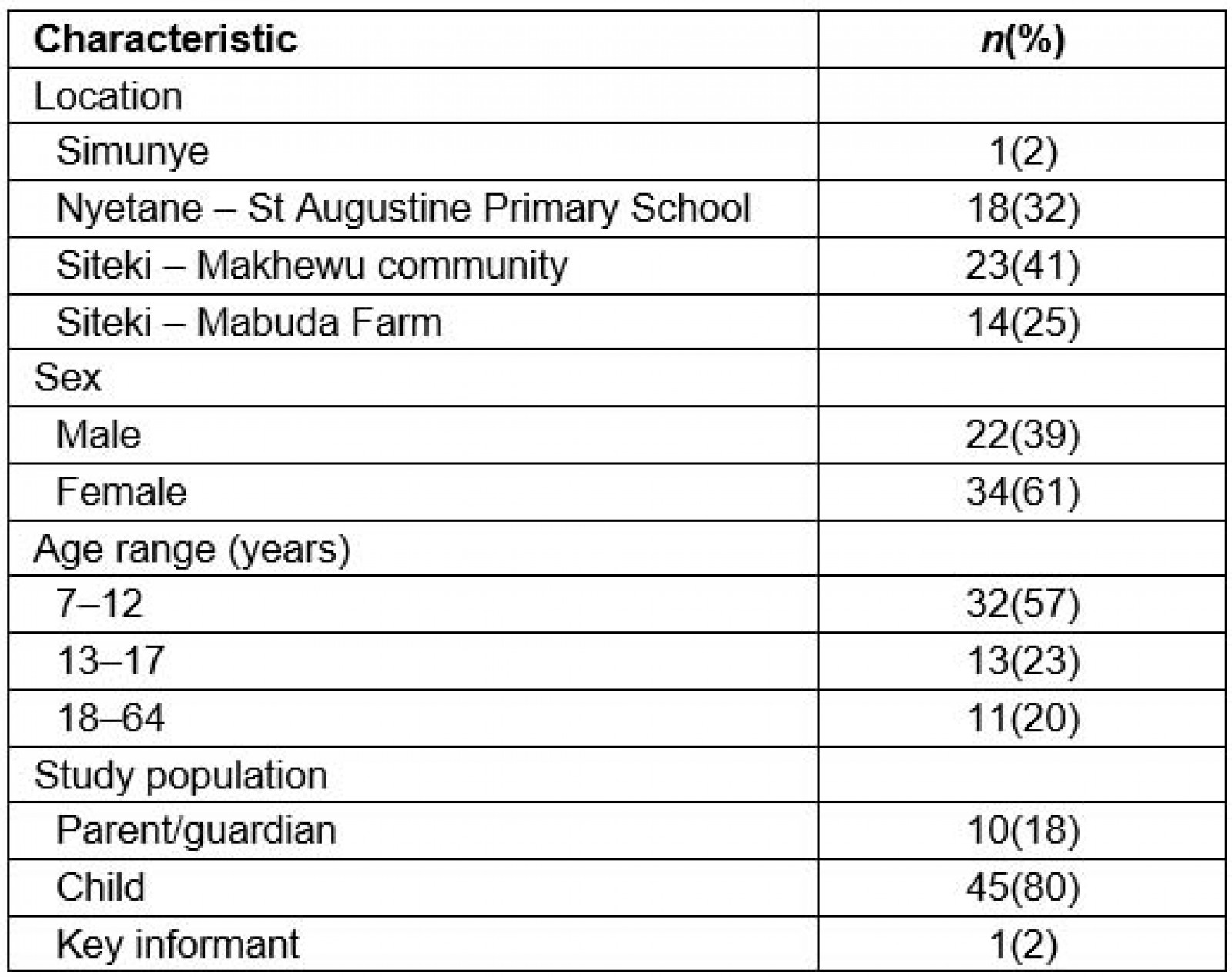
Table 2: Domains, themes and subthemes derived from qualitative analysis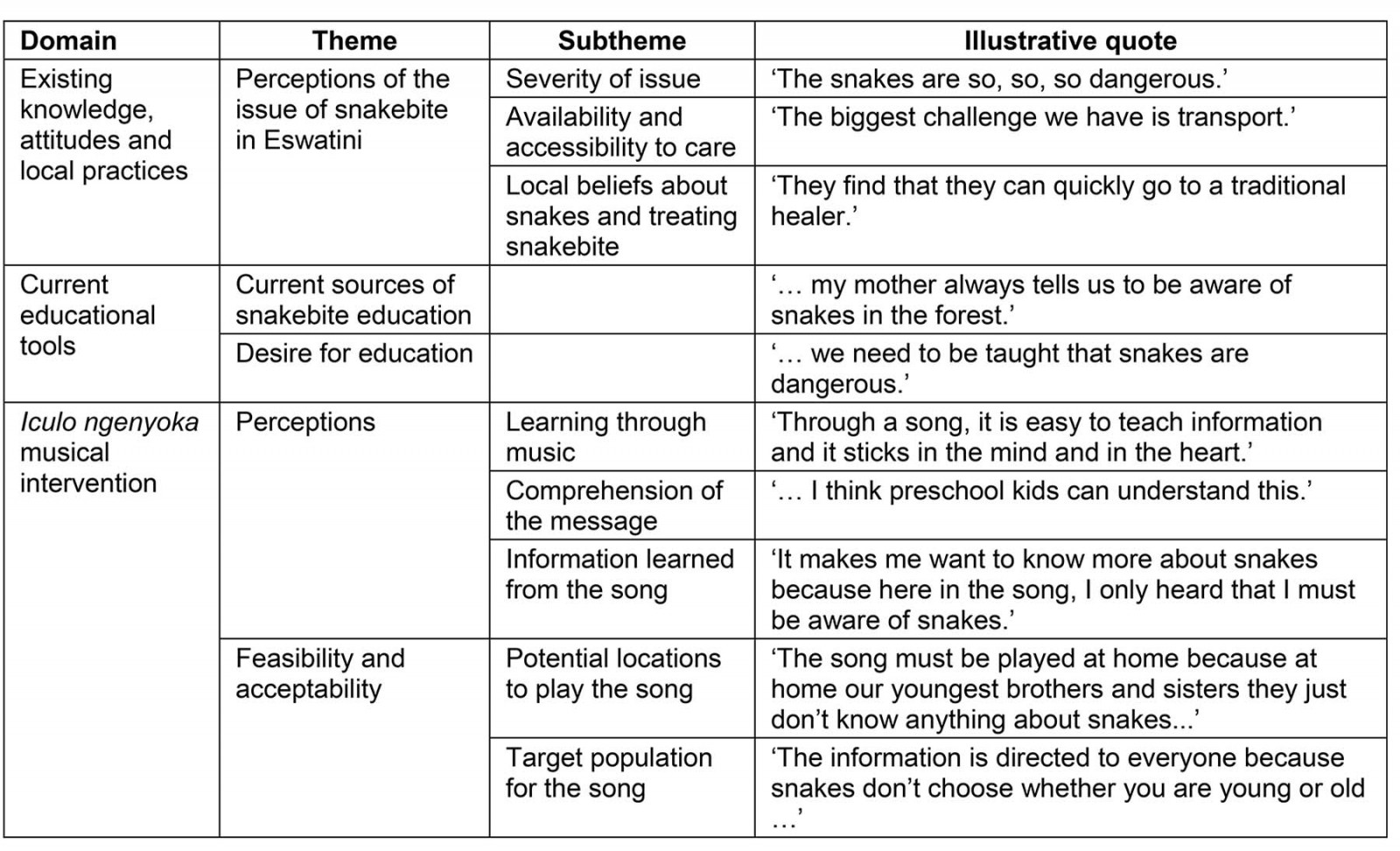
Perceptions of the issue of snakebite in Eswatini
Severity of snakebite as a public health issue: During the interviews, many participants highlighted the severity of snakebite in their communities. They described how they had seen snakes in their homes, at their school or on the road. Many participants knew someone who had died because of a venomous snakebite, or had experienced a snakebite first-hand. The key informant, a local snakebite expert, described the severity of snakebite and the populations most vulnerable:
If you talk to a Swazi, snakebite is terrible. You either die or you lose a limb, and it is just accepted … In Africa, we estimate over 50,000 people every year die from snakebite. And that is not the 200,000 people that lose a limb, or are permanently disfigured. [Snakebite envenoming] is a poor man’s disease, so it affects those people without a voice. That is our biggest challenge. It is the rural person who sleeps in a traditional home, on the floor or even on a bed, in a house that is not protected, that does not have air conditioning and a screen door that closes behind you as you walk out. Statistically, 70% of our victims were bitten whilst they were sleeping.
The St Augustine Primary School in Nyetane is in the heart of the Lowveld region, which was noted by local snake experts to have one of the highest rates of snakebites in Eswatini. Several interviewees from the St Augustine Primary School had personal experiences with snakes or knew someone affected by a snakebite. A girl (aged 12 years) from the school described her experience of losing her family members because of a snakebite:
I have lost two relatives to two snakebites. The first was my aunt. She got a snakebite on her thigh and she passed away. The second one was my grandmother. The snake bit her on the leg and they tried to rush her to hospital but she also passed away … The snakes are so, so, so dangerous.
While the majority of participants perceived snakebite as a serious issue, some participants described snakebite as an insignificant issue in their community. A girl (9 years) from the Makhewu community stated, ‘I think they [snakes] are not a serious problem because I have never seen a snake and I haven’t heard of anyone bitten by a snake. They are just not a problem at all.’ It was apparent that participants who had seen snakes or knew someone that was inflicted by a snakebite perceived the issue of snakebite differently than participants who had never seen or had an experience with snakes in their community.
Availability and accessibility of care: Rural communities experience a multitude of challenges to accessing treatment for snakebite. Many participants highlighted the main barriers they perceived to accessing medical care, such as inadequate medical care to treat snakebite and transportation barriers to hospitals equipped with antivenom. A mother (29 years) from the Makhewu community stated, ‘Since our area is a bit far from hospital, we don’t have transport which we can rely on.’ In the dire circumstance that a vehicle could not be found, ‘the only option you have is to take the person by wheel barrow to hospital, or just carry him or her by your back,’ according to a mother (57 years) from Makhewu.
Several participants also described various challenges snakebite victims may encounter if they do reach a hospital. A girl (13 years) from Mabuda Farm highlighted a shortage of antivenom in hospitals:
You may find that in the hospital there are a lot of people that are suffering from snakebite, so the antivenom, they are using it a lot. You find other clinics don’t have the antivenom because you may find the nurse who is in charge of that hospital doesn’t give a serious attention about snakebite.
Not only was a shortage of antivenom a critical barrier, but physicians were often not properly trained to diagnose and treat snakebite envenoming. The key informant contextualized the challenges snakebite victims may experience in a hospital setting:
This year alone, we have had six or seven deaths when the doctors have said, ‘Oh, I didn’t have antivenom, so what could I do?’ You say, ‘Ventilate [Advanced Life Support], all you need to do is ventilate if you don’t have antivenom … You don’t need to say your goodbyes and take your victim home.’
The current antivenom in Eswatini is supplied by the South African Vaccine Producers, which has triggered an allergic reaction in many cases. In the instance of an allergic reaction, antivenom administration must be paused, which may allow the snake venom to continue to harm the patient. It may also hinder a doctor from administering enough vials of antivenom to neutralize the snake venom.
The interviewees perceived many challenges to accessing appropriate treatment for snakebite. When asked to describe the greatest challenge to accessing antivenom, a mother (58 years) from the Makhewu community, who had been bitten by four different snakes in her life, explained, ‘It is the lack of knowledge … Nobody teaches the children what to do whenever they are bitten by a snake.’
Local beliefs about snakes and treating snakebite: In discussions of what to do in the event of a snakebite, many participants highlighted incorrect first aid techniques such as drinking aloe water or coconut oil, eating mud and most notably, tying a tourniquet above the bite site for any snakebite. Some participants described how snakebite victims may seek treatment from a traditional healer, who would treat snakebite with umutsi: various herbs, ground bark and sometimes animal parts. Some participants described how the bite site would be cut and umutsi would be placed in the cut to treat a snakebite. Participants believed the umutsi would be a form of first aid, and that many snakebite victims would eventually seek treatment at a hospital. This practice can not only delay appropriate antivenom administration, but also cause infection and further complications.
Because access to medical facilities was perceived as a significant challenge, traditional healers were perceived as the next best option to a hospital. A mother (47 years) from Makhewu stated, ‘Since there is a scarcity of transport, here you find that they look for closer options. What else can they do? Calling a taxi may never come … so they find that they can quickly go to a traditional healer.’ When asked about snakebite victims seeking treatment from a traditional healer, the key informant described, ‘It is just out of desperation because it is the only option. If we could improve getting the victims to a medical facility quicker we would be able to make a big difference with the outcomes of snakebite.’
Current sources of snakebite education
Interviewees identified the sources of information about snakes in their community. The majority of the knowledge they learned came from information from their families, friends, teachers, first-hand experiences with snakes, media or stories they heard of someone getting bitten by a snake. Many of the participants described learning about snakes at home from their elders. When asked where she had first learned about snakes, a mother (58 years) from Makhewu explained:
Whenever the elders killed a snake, they would call the children to come and see it. They would educate us that if we ever see this animal, it is so dangerous … we must run away … I also experienced seeing my friend being bitten by a snake. Unfortunately, she passed away due to lack of knowledge because we didn’t know what to do.
A girl (12 years) from St Augustine Primary School described learning about snakes from her mother when she did household chores: ‘At home we usually collect firewood and my mother always tells us to be aware of snakes in the forest.’ Many participants explained how their knowledge came from personal experiences of snakes coming into their homes or seeing them on their way to school.
Desire for education about snakes
The key informant was devoted to implementing community engagement programs and rescuing snakes from people’s homes. In addition to educating communities, the key informant strived to educate medical professionals about properly diagnosing and treating snakebite envenoming. This educational process entailed compiling diagnosis and antivenom treatment guidelines for local venomous snake species and conducting educational symposiums for medical professionals around the country. When asked about the best strategies to educate communities about snakes, she responded:
It is just community, it is just talking, it is getting out there and talking to schools, trying to tell them what you would do once again to prevent the snakes from getting into your home. What you do in case of snakebite. So, education is key. You have to educate.
Many of the participants perceived snakebite as a serious issue in their community, yet minimal educational resources were available to them. Despite the current educational tools and engagement programs, many of the participants described the demand for more information about snakes in their communities and schools. A boy (12 years) from St Augustine Primary School stated:
I think there is a need that we must be taught about snakes because not everybody has knowledge about snakes. It is not something you can play around with so we need to be taught that snakes are dangerous.
When asked to elaborate on the information they wanted to know about snakes, many participants were curious to understand the difference between the local venomous and non-venomous snakes, why it is important to have snakes in the ecosystem, first aid treatment in the event of a snakebite and how to prevent snakes from entering homes.
Perceptions of Iculo ngenyoka musical intervention
Learning through music: Overall, the musical intervention was perceived as an effective and culturally relevant tool to spread a message about snakes. The children and parent/guardian interviewees predominantly agreed that music was an engaging and effective way to learn. Many interviewees highlighted the ease and enjoyment of teaching and learning a message through music. A father (59 years) from Makhewu remarked, ‘Through a song, it is easy to teach information and it sticks in the mind and in the heart.’ A boy (15 years) from Mabuda Farm stated, ‘I think it [music] is the best way of passing on a message because most of us really like music … and it is easy to remember lyrics in a song … you remember everything.’ Interviewees also described the simplicity of learning a message through a song, as well as the ability to repeat a song to fully understand the message. A girl (14 years) from St Augustine Primary School said, ‘… you can repeat the song again and again and again if there are some words you don’t understand. At the same time, it is fun to learn through music.’
Many interviewees explained that they preferred to learn through music because it was convenient to listen to a song. They described how they can listen to a song while doing chores, cooking, walking to school or riding on public transport. As a girl (13 years) from Mabuda Farm explained, ‘you don’t have to open a book, you just have to listen.’ Several interviewees described how not every child in their community has an opportunity to attend school. The interviews revealed that music may be an effective educational tool for these children. A girl (16 years) from Mabuda Farm described that:
… everyone is eligible to music. While not all of us get the opportunity of being in class and having somebody teach you. So, the music is the best way because at any time, even at home, everywhere, even along the way, you can listen to your music, so the information is just passed easily than just being in class.
The key informant highlighted the use of music for the purpose of education:
It is probably one of the most effective tools is to sing and dance … It is the way Africans pass down everything – their history, their stories. That is part of who they are – is song.
Interviews revealed contrasting opinions regarding education through music. Several participants contextualized how they preferred to be lectured by a teacher in school, as opposed to learning messages through music. A boy (12 years) from St Augustine Primary School explained:
I would prefer to be lectured because … if I do have a question I would ask it right away, but with music, like right now, I have questions like what I do if I get a snakebite. So, music I can’t ask a question at that time.
Comprehension of the message: Because the song was sung in Zulu and all the participants spoke siSwati and/or English, it was critical to understand if the participants understood the song. The participants were asked to describe their understanding of the song’s message and if there were words they did not understand. The interviews revealed that the majority of the participants expressed understanding of the lyrics and the message from the Iculo ngenyoka musical intervention. During the interviews, participants explained how siSwati and Zulu are very similar languages, with minor differences in tones and clicks. A woman (23 years) from Makhewu stated, ‘It is very clear and understandable. I think preschool kids can understand this.’
Conversely, some interviews revealed that several child interviewees did not fully understand the first and last verse of the song. A girl (10 years) from St Augustine Primary School stated, ‘I didn’t get some of the information from the first verse. But all the other things were clear.’ It was not defined which words were not fully understood. However, when the song was repeated by request, the children expressed clearly understanding every word of the song.
Information learned: While many participants expressed enjoying the rhythm, the beat and the voice of the singer, many described how the message of the song was the most important. Several interviewees described how the information portrayed in the song was not necessarily new information to them. However, they perceived the song as a tool to raise awareness about snakebite. In Makhewu, a mother (58 years) stated, ‘… the song is the best way to use in raising awareness about snakes because it has got such an important message which is loud and clear to everyone.’ Several of the child participants perceived the song as a tool to raise awareness about snakes and felt that the song initiated a desire to learn more information. For example, a girl (7 years) from Mabuda Farm explained, ‘It makes me want to know more about snakes because here in the song, I only heard that I must be aware of snakes.’
Several participants, including children and parent/guardian participants, did learn new information from Iculo ngenyoka. They expressed how they learned that snakes live in grass, bushes and under rocks, and to tell an elder whenever they have seen a snake. One participant learned from the song that snakes can bite. A girl (14 years) from St Augustine Primary School explained, ‘I only knew that they only spit the poison, not that they can bite you.’ Several of the child participants described how the song had changed their opinions about their actions when they would see a snake. They expressed how their initial reaction to a snake was to attack and try to kill it, but from the message in the song, they learned to report a snake to an elder, such as a parent/guardian or teacher. A girl (15 years) from Makhewu stated, ‘What I knew all along that whenever I see a snake, I must just take a stick and attack the snake, but now I know that I mustn’t do that. I must report to an elder.’
Feasibility and acceptability of Iculo ngenyoka musical intervention
Potential locations: Many of the participants perceived the song as an acceptable tool to raise awareness about the dangers of snakes in their community. Many of the interviewees described how the song would be appropriate for broadcast on the radio, television, in a hospital setting, in a homestead, and taught in schools. The interviewees conveyed that many homesteads owned radios, televisions, a phone or other device that could play the song. Many participants believed the song should be played in the homesteads for their elders and youngest siblings to learn the message. A mother (29 years) from Makhewu stated:
I can play the song in the homestead … I can even raise the volume so everyone can listen to it, even the neighbors so that they can also be aware. And the children can easily get the song. They can be singing it even along the road. Teaching their friends, the song about the snake.
All of the child participants described how the song could be taught at their schools, so their peers and teachers could learn the message from the song as well. For example, when asked about the acceptability of playing the song at school, a boy (14 years) from Makhewu responded, ‘It is best that they must play it in our school because all the other students can also enjoy the song as much as we enjoyed it.’ Some interviewees believed the song should be played on the radio so everyone could listen to the message. As a mother (57 years) from Makhewu stated, ‘The song can be played everywhere because we all need to be aware of snakes.’
Target population: Interviewees were asked to describe who they felt would be the ideal target population for the song. While participants agreed that the song was primarily tailored for young children because of the nature of the message, they also suggested that most age groups would enjoy listening to the song. The key informant stated:
I think it’s something that would be appreciated through all the age groups, but probably for the younger because go and tell your mom, tell your dad, tell your teacher, but it’s probably something that could be sung by anybody, it is a lovely tune, it has a lovely beat.
A mother (57 years) from Makhewu believed the song was appropriate for every age group: ‘The information is directed to everyone because snakes don’t choose whether you are young or old, they just attack everyone.’
Discussion
The findings from this study highlight the tragic reality of snakebite envenoming in communities in the Lubombo region and a distinct gap in education about snakes. The majority of snakebite education was taught by the elders in a home setting. For some interviewees, their knowledge about snakes originated from school, television programs or personal experiences with snakes. However, the amount of information conveyed about snakes was typically minimal: many of the interviewees knew that snakes were dangerous but they often did not know why, or about the type of snakes that present a serious threat to humans. This study’s findings suggest an urgent need for further education, especially in rural communities and school settings.
Music was perceived as a culturally acceptable, engaging and memorable method to disseminate a message about snakes. The upbeat melody, familiar language and valued message resonated with the children and elders alike. Songs occupy an important place in African oral traditions and have been used for centuries to pass health, agricultural and cultural messages from generation to generation15. Anecdotal research highlighted that local populations in Eswatini used song and storytelling to teach children about the danger of lightening strikes in the region, and to sleep under a bed net to prevent mosquito bites.
Similarly to previously studied health education entertainment tools, the repetitive nature of Iculo ngenyoka was found to be an important design element; repeated words and phrases increase the opportunity for the message to connect with its target audience21. The NuRhyme structure provides a natural progression for listeners to learn the places where snakes may be found, why it is important to be aware, and an action to take when a snake is encountered. Previous literature regarding nursery rhymes suggests the structure of these rhymes may be beneficial to a child’s cognitive development due to pattern recognition, and easy recall and memorization abilities21. Because Iculo ngenyoka was relatively short (1 minute, 43 seconds), the participants wanted to repeat the song to hear the message again. Previous health education entertainment literature has shown that repeated playing of the song increases the probability that the message will be retained21,22. Although it is not proven whether a retained message translates into behavioral change and ultimately preventable snakebite accidents, this study is an important start to understanding how innovative health promotion tools can be deployed to mitigate health burdens such as snakebite, not only in Eswatini, but worldwide. The structure of a NuRhyme may be applied potentially to other health burdens and languages. To exemplify the potential of deploying similar nursery rhymes in other locations burdened by snakebite, the same song was translated in Tamil (Appendix I). In India, music has been used for health promotion in children in a variety of studies23-26.
Study limitations
This exploratory study had several limitations. Iculo ngenyoka was not performed in siSwati to correspond with the primary language spoken by the participants. However, based on the results of this study, Zulu and siSwati are very similar languages and the Iculo ngenyoka song was understood by all participants.
The English section of the recorded interviews was transcribed without a siSwati interpreter. The English translation between the interviewer and interpreter during the audio-recorded interviews was used to transcribe the data. This may have resulted in imperfect translations and imperfect word-for-word transcription. However, this was the most appropriate method for transcribing the large number of interviews, given the budget and time constraints for this project. For quality assurance, the audio-recordings were reviewed by each translator before the transcription process to ensure they were clear and the data were accurate.
With regard to the participant’s responses during the interviews, exposure to the song prior to the interview, social desirability bias and the tendency of participants reporting answers to questions in a socially acceptable manner may have biased the results27. For many participants, it was their first experience participating in research study and being interviewed in a formal one-on-one or small focus group setting. Additionally, participants were notified during the consent process that they would receive incentives for their time and participation in the study. This may have introduced incentive bias. The student researcher emphasized during the consent process that he had no influence in the song and was a neutral party, in efforts to mitigate response bias.
A mixture of convenience, purposive and snowball sampling techniques was used for this study. This may have resulted in selection bias of the participants28. Interviews were only conducted in four settings that had the highest prevalence of snakebite, so the findings may not be representative of Eswatini as a whole. However, snakebite is largely neglected as a public health issue in the country, so this exploratory qualitative study intended to understand the opinions about the Iculo ngenyoka musical intervention in communities facing the greatest burden of snakebite. It was not intended to draw conclusive opinions potentially applicable to Eswatini as a country.
Strengths of research
The exploratory study is the first known qualitative study conducted to understand the attitudes and perceptions of a musical intervention aimed to educate communities in Eswatini about the dangers of snakebite. The number of childr participants in this study surpassed initial target numbers, which allowed for an abundance of data to analyze, and for strong themes to emerge. The interviews revealed the desire for more education about snakes, which signifies the need for more creative strategies to educate the communities in the Lubombo region about how to prevent and treat snakebite accidents.
Recommendations for implementation
The findings from this study suggest that the Iculo ngenyoka song offers an acceptable and portable medium for educating children about snakebite and increasing awareness to reduce the burden of snakebike envenoming in the region. The message conveyed in the song was often perceived by interviewees as common knowledge about snakes, although some expressed they had learned new information from the song. The musical intervention may be appropriately deployed as a useful tool to raise awareness about snakes in communities. Based on these findings, it is recommended to integrate Iculo ngenyoka into existing community engagement programs, communities, school curriculums, and radio and television broadcasts.
Navigating lifestyles and living conditions around venomous snakes is particularly challenging for rural populations living in the Lubombo region because their livelihoods depend on agricultural yields, and their living conditions expose these communities to snakes. The findings suggest musical interventions are worthy of further investigation, and it is recommended to discover if a retained message from a song translates into preventable snakebite accidents, and if group participation is an effective approach to enhance knowledge retention of a song.
Conclusion
This study is one of the first to explore the potential of a musical intervention in educating vulnerable communities in Eswatini about snakes. The study provides preliminary evidence about the impact of musical interventions as tools to educate communities about snakes. The results emphasize the demand for education and the potential use of Iculo ngenyoka and similar musical tools as vessels to raise awareness about snakebite in Eswatini and possibly in other vulnerable communities around the world.
Acknowledgements
The authors thank Eoin Harrington for creating Iculo ngenyoka and the Nurhymes concept for the purpose of public health education for children, globally. Thank you to Gideon Bhendile for volunteering his time to record the Iculo ngenyoka song and sharing his talents for the purpose of research and global health education. Thank you to Stephen Samuel for translating the ’Snake song’ in Tamil and Telugu and Simon Samuel for sharing his talents to compose the ’Snake song’ in Tamil. Thank you to our interpreters Thobani and Temanteni for all your hard work and positivity. Thank you to Darah Boucher from the Peace Corps for all of your assistance in Nyetane. Thank you to Shannon Fuller for your advice and guidance regarding qualitative methodology. Thank you to Nicole Santos for your critical eye and guidance throughout the year. Lastly, thank you to faculty, teaching assistants and 2017–2018 cohort at the Department of Global Health Sciences, University of California, San Francisco for your support. Telugu translation assisted and proofread by Anjani Devi Errama, Vidhyaprakash Rajendran and Juttiga Uday Kiran.
References
appendix I:
Musical intervention lyrics (English, Zulu, Tamil, Telugu)
English: https://youtu.be/0XnJmghos-w
Tamil (translated by Stephen Samuel): https://youtu.be/VtHzXITMrYk
You might also be interested in:
2015 - Developing a culturally competent, sustainable rural model for diabetes prevention
2006 - Violence in rural communities: youth speak out!
2003 - Recruiting foreign doctors to South Africa: difficulties and dilemmas