


Introduction
Adolescence is a significant period of transition where lifelong health behaviour habits are consolidated1-3. Many modifiable behavioural risk factors affecting current and future health and wellbeing can be positively influenced at this time1,4. The primary healthcare sector is pivotal to health over the life course. However, adolescents are underrepresented in Australian general practice5,6. Barriers to adolescent primary healthcare access are complex and include social, behavioural and geographical issues as well as organisational and systemic barriers.
Previous studies have examined these access issues in depth. There is general agreement internationally that youth-specific health services are not easy to implement and sustain7. The Longitudinal Study of Australian Children (2017) reported location, fees, stigma and embarrassment as significant barriers to appropriate and timely care for adolescents4. Gender and peer stigma is a particular barrier for adolescent males8. International research depicts rural adolescents as having higher unmet primary care needs and fewer preventative care visits than their metropolitan counterparts9,10. An Australian rural youth survey (n=177) indicated 64% of adolescents required transport to attend appointments and 71% felt their general practitioner (GP) visit would not be confidential3. The school setting was identified as a potential health enabler in a rural Canadian study involving 288 students11.
Organisational barriers can prevent GPs from delivering adolescent health care and appropriate health promotion12. These include limited appointment times due to the fee-for-service structure, administration staff ability to be sensitive and respectful to adolescent needs, and lack of adolescent understanding of GP confidentiality requirements3,6. Overall, Australian general practice has inadequate adolescent health expertise, difficulty communicating with young people and is hampered by poor knowledge of relevant, accessible referral pathways for adolescent support services5,13. There is evidence that this situation is repeated in rural communities worldwide7.
Developing appropriate adolescent-friendly models of care to address the primary healthcare needs of young people is essential. The Doctors in Secondary Schools program is an important step in catering to context-specific adolescent health and wellbeing needs. This article provides a project report on one rural school’s implementation of this state-funded initiative as a rural youth model of primary care. The description applies a pragmatic approach that focuses on ‘what works’ to examine contextual program implementation and quality improvement activities, using secondary data14-16. The secondary data comprise the practice nurse’s log of implementation actions, monthly project activity reports, publicly available area-level population characteristics and school statistics, and reports from concurrent local initiatives.
The specific background of this program provides important context for international organisations or individuals who may wish to implement a youth-specific health service. The Doctors in Secondary School program is a Victorian Government initiative that commenced in 2017 in conjunction with the Department of Education and Training17,18. In recognition of the difficulty in implementing and sustaining youth-specific services, the broad objectives of the statewide program are to make primary health care more accessible to secondary students, provide assistance for adolescents to identify and address health concerns early, and reduce the pressure on working parents. These objectives aim to contribute to achieving the state government department targets of ‘happy, healthy and resilient kids’ by improving access to health services for young people17.
Government selection of schools for implementation
The selection of secondary schools for program funding involved metropolitan and non-metropolitan sites. Schools responded to selection criteria and were required to demonstrate the health and wellbeing needs of their student population along with a willingness to build community relationships and commit to student health and wellbeing. Applications for program funding were managed through Victoria’s six primary health networks (PHNs) via the commissioning process17,18. Involvement of the PHNs facilitated engagement of the primary health sector, medical centres, GPs and practice nurses18.
Government implementation timeline
One hundred schools across the state of Victoria were involved in the three-stage implementation process. The first stage involved 20 secondary schools commencing the program in term 1 of 2017. The second stage added 40 schools in term 3 of 2017. The final stage added a further 40 secondary schools in term 1 of 2018. Each successful school partnered with a general practice clinic to provide the service on school premises and to supply the GP and practice nurse to operate the service.
Context-specific school implementation
The program commenced at the school that is the focus of this report in the final roll-out stage in term 1 of 2018. The program is delivered in school by a local general practice with an active clinic co-located within the township’s small rural health service. The in-school clinic is staffed by one of the local GPs and a practice nurse who is employed in a senior position at the local rural health service.
Key local government area (LGA) population characteristics are important to highlight a context-specific profile. The LGA population was approximately 29 300 at 2016 census and the school site township population at 4500 people19. The total school population was 255 students in 201720. The student population consists of young people from the town and other students who travel by bus from outlying areas throughout the shire. LGA-level data19,21, compared for two points in time (2011 and 2016), showed a declining 0–19 age group population, with the potentially non-working population (children and the aged) being nearly equal to those potentially employed (Table 1).
Table 1: LGA population characteristics compared, 2011–201619
Context profile
The LGA has high disadvantage. In 2016, the shire was ranked 178th out of 544 LGAs listed on the Socio-Economic Index for Area, placing the shire in the bottom third of most disadvantaged LGAs in Australia19,21. There is a lower than state average medium weekly household income and lower rates of educational attainment (2011 and 2016). Educational attainment for the shire is failing to keep pace in closing the gap when compared (2011 and 2016) to state rate rises: shire rate increased by 8% but state rate increased by 24% (Table 1).
The level of disadvantage facing those in the LGA where the school is located suggests that families in the school contend with challenges that influence the social determinants of health. Socioeconomic status is strongly associated with health literacy levels, with low health literacy a predictor of health status and future health outcomes22,23. Health literacy is a complex issue; it involves having the skills and resources needed to manage health and minimise disease23.
Disadvantage is similarly reflected in the local school Index of Community Socio-Educational Advantage (ICSEA). The ICSEA scale allows comparisons among schools with similar students. As such, it provides an indication of the socio-educational backgrounds of students. It is not a school rating nor relevant to staff, school facilities or teaching programs20. The ICSEA scale for the school at this rural site showed that, in 2017, more than half (58%) of students were in the bottom quartile of disadvantage20.
Ethics approval
The present report utilised secondary data with no identifying information, and content was carefully considered to uphold ethical responsibilities. The use of this secondary data did not require an ethics application. Processes adhered to the ethical obligations involved in the National Statement for Ethical Conduct in Research.
Results
Processes and outputs of the school clinic
The program commenced in February 2018, and has provided 33 clinics and 332 appointments to the end of November 2018. This equated to 102.33 hours of GP service. There is no process in place to record student time with the practice nurse, the role having a set number of hours across all duties. The school clinic is open twice a week during school terms and takes appointments from 9.30 am to 2 pm. Scheduled and unscheduled (drop-in) appointments are accommodated. There has been a 9% (n=30) rate of non-attendance (‘no-show’) and cancellations for appointments over the school year. The reasons for non-attendance are recorded as cancellation, other school obligations, school absenteeism, and appointment ‘no-show’. The practice nurse indicated that common reasons for seeking GP support included routine medical issues such as immunisations, blood tests, asthma, headaches, abdominal pain, skin issues and wellbeing issues such as depression, anxiety, behavioural concerns and poor sleeping. Students aged 14–18 years were the most frequent users of the clinic.
Summary of year 1 of the school clinic
An overall summary of clinic attendance figures by month was collected by the practice nurse from commencement of the program in February 2018 to the end of November 2018 (Table 2).
Table 2: Clinic data summary 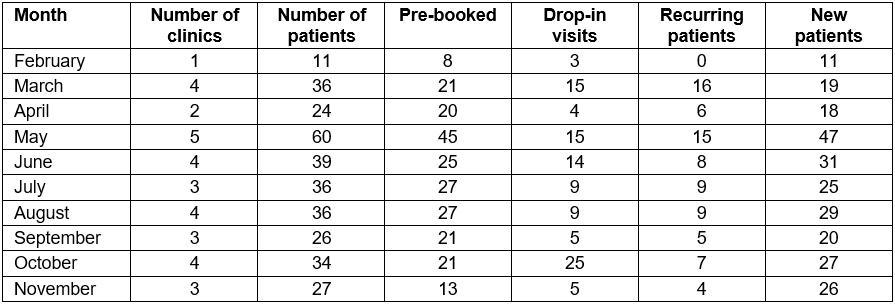
Appointment duration per patient with the GP averaged at 18.5 minutes. There were an average of 7.3 recurring clients per clinic, 2.6 new patients, 7.3 pre-booked clients and 2.8 drop-ins per clinic. The longer appointment is a critical need for young people, with previous studies indicating average GP appointments of 14.8 minutes24. This school GP is providing young people with approximately 4 minutes longer per appointment. Additionally, previous youth health research found that difficulties obtaining appointments at convenient times are a major barrier to primary healthcare accessibility25, hence the value of the drop-in component of this service.
A community approach to access and needs identification
The clinic practice nurse, who is also a senior nursing staff member of the local rural health service, has sought to be responsive to identifying and actioning student health and wellbeing needs. Practice nurses can improve patient knowledge, establish trusted health advice relationships, increase youth compliance and reduce GP workload to support time-limited GPs26. According to the practice nurse program reporting documents, a community development approach was taken to meet identified gaps and access issues.
Fruit consumption was an issue identified by talking to students and by practice nurse involvement in a youth survey from a concurrent local project. This was also reflected in LGA adult population health data27, which showed less than half (49%) have two or more fruit serves per day. The practice nurse has taken the initiative to provide fruit on clinic days. This has been highly successful, starting with the provision of 32 pieces freely accessible outside the clinic door. Due to demand this has now increased to 50 pieces of in-season fruit on each occasion. There have been no reports of discarded fruit in the broader school environment. This small initiative could positively reinforce fruit consumption and create longer term habits for increased fruit intake.
Service access and referral pathways are a common concern identified in the literature5,6. During the implementation period of the school clinic it was unclear what types of appropriate services were accessible to the school population. The practice nurse completed a wide-ranging audit to further understand the youth service support environment. Direct visits were made to local regional services to gain a clearer understanding of the type of services and model each offered. The GP and practice nurse identified the challenges in making referrals to regional services whose operating hours conflict with school attendance for students, with after-school appointments impossible due to rural distance and travel time. In addition to the challenges of missed school attendance to attend appointments, limited public transport is available for these students to negotiate the distance to a regional service centre. The GP and practice nurse continue to advocate and negotiate for services to visit locally on a regular basis.
Practical and often sensitive consumables such as sanitary items and condoms were identified as not readily accessible to young people but could be provided by the practice nurse at the school clinic. These types of resources and associated information from a health promotion or prevention approach are essential to increase health literacy in young people. Low health literacy is associated with poor health, incomplete understanding of health problems, reduced treatment and management, and greater risk of hospitalisation2,3,25. In addition, the practice nurse has collected a range of youth-friendly service brochures and information pamphlets, which are available for students at the school clinic.
The practice nurse has also made strategic links to current initiatives in the local adolescent primary healthcare space. Such an example is a small project grant from a financial institution to the health service, which aimed to support disadvantaged rural youth. A point to highlight (related to service access) is that the practice nurse worked closely with the grant project team advocating for the Centrelink mobile unit (related to social security services) to visit locally. The practice nurse had recognised students were unclear about the processes to gain their own Medicare card or what types of support options were available from Centrelink. This issue has been previously identified in Australian research, which found many young people are unaware they can hold a Medicare care independently from the age of 15 years6. As a result of this advocacy, the Centrelink mobile unit visited the township in November 2018.
Discussion
This rural Doctors in Secondary Schools program has identified primary healthcare needs for local adolescents. Young people have specialised needs, and youth-friendly services must be accessible, acceptable, equitable, appropriate and effective28. The practice nurse has taken an approach that considered the importance of interrelationships, particularly across the local service and community environments, to understand and meet adolescent health needs. It is important for the future that the practice nurse works closely with the existing education department funded school nurse position in health promotion planning. This approach is readily transferable, as the crucial aspect is consideration of context and pre-existing relationships. Adolescent health is a predictor for future population health, so addressing health issues and behaviour early can improve the immediate quality of life for young people and is socially and economically more effective than dealing with enduring problems in adulthood24,29. This is highly relevant due to the increasing burden of chronic disease and the continued upward trajectory of chronic disease levels in Australia and worldwide7,30.
Limitations and recommendations for research
The Doctors in Secondary Schools program is an important state government strategic initiative and a model of care that provides an exemplar of replicability. Parent satisfaction, the perceptions of students and understanding health outcomes could be the focus of future research. Kang et al highlighted the need to go beyond process evaluations and output reporting to increase the evidence base for youth health5. A key lesson in describing this program through secondary data and practice nurse actions highlights the need for government departments as funders to understand context-specific implementation factors rather than relying solely on output reporting.
As a project report this article has limitations; it is critical that further research is now conducted in this area with primary data to understand implementation barriers and enablers, outcomes and effectiveness for all involved.
Conclusion
This Doctors in Secondary Schools program has provided a rural school population with access to GP services. It is an important program for students in the local township and also for students who travel by bus from outlying areas. These rural students previously had limited opportunities for their health needs to be conveniently addressed. The practice nurse and GP have considered the care needs of these adolescents and have actively advocated for increased adolescent-specific services along with providing a range of information and resources to improve health literacy and wellbeing for this cohort. As discussed by May and Finch, successful implementation of programs requires contextual integration, skill set workability and relational integration31. These are all essential elements for embedding new models of care in rural primary care settings and can be applied across international contexts.
Acknowledgements
The authors would like to thank the local health service for supporting this project report and assistance with secondary data sources and project reporting information.
This report has been supported by the Australian Government Department of Health through the Rural Health Multidisciplinary Training Programme. This research did not receive any specific funding.
References
You might also be interested in:
2013 - Using Portable Health Information Kiosk to assess chronic disease burden in remote settings