







Introduction
The current SARS-CoV-2 coronavirus epidemic (COVID-19) and the confinement strategies aiming to stop the spread of the virus, are severely disrupting physical activity1, mental health2, diet3 and economies4 globally. The catastrophic effects of COVID-19 on employment, working hours and incomes are as evident in Latin America as they are throughout the world. During the three first quarters of 2020, the estimated decline in working hours was 20.9%, while employment incomes decreased by 19.3%5.
The most affected groups have been those that, due to the type of their work, cannot telework, and rural areas cannot escape this difficult reality. The rural population from Latin American countries would reach 120.6 million people, representing 18.5% of the total population6. Among rural workers, 76.2% are subject to informal labor conditions and employed in very low productivity economic units5. This informality, together with the stress associated with confinement, the difficulty selling products produced in the countryside, among other financial problems7, may negatively affect aspects such as psychological condition, eating habits and body weight gain among Latin American rural populations.
It is also known that mental health influences people's diet and vice-versa8-10. For example, it has been observed that stress is associated with a decrease in diet quality and that high-fat diets induce anxiety, anhedonia and depressive behaviors9,11,12. However, little is known about how mental health influences diet quality in the rural world, let alone in the context of the COVID-19 pandemic confinement. The rural population has less access than the urban population to basic services. It is possible that during the pandemic and, especially, during the extensive lockdowns (which affected the movement of food and greater isolation of the population), they could be exposed to a negative quality of food and also have symptoms of appetite and anhedonia. The objective of the present study was to determine the relationship between symptoms of anxiety and/or anhedonia and diet quality during confinement due to COVID-19 in rural populations in Latin America.
Methods
A multicentric, cross-sectional study was conducted between 15 April and 4 May 2020. The present manuscript depicts a secondary analysis of data collected for the approved study on ‘Anxiety, anhedonia and food consumption during the pandemic in Ibero-America’.
Participants
Citizens invited to take part in the study were from 11 participating countries: Argentina, Chile, Colombia, Costa Rica, Ecuador, Guatemala, Panama, Paraguay, Peru, Uruguay and Mexico. All participants in the primary study (n=10 552) were asked if they lived in an urban or rural area, the latter being selected for the present analysis. All the participants had to be aged over 18 years and accept the informed consent before accessing the online survey. Exclusion criteria were as follows: pregnant and/or breastfeeding (first 4 months); receiving pharmacological treatment or psychotherapy for depression, anxiety disorders, stress and/or mood disorders; and receiving nutritional management prescribed for the treatment of pathologies.
Procedures
All participants voluntarily and anonymously completed the survey through different social media platforms and networks such as Facebook, Instagram and Twitter, and through personal as well as corporate email accounts. The survey was conducted using Google Forms. It was applied once and was self-administered. In order to determine the minimum number of participants to be surveyed by country, sample sizes were calculated on the basis of the statistical analyses of association and comparison according to the groups to be studied, using the software G*Power v3.113.
Virtual survey
The virtual survey consisted of questions extracted from validated instruments designed to assess diet quality and mental health of participants. Three instruments were included: a food intake questionnaire, the Beck Anxiety Inventory (BAI) and the Snaith–Hamilton Pleasure Scale (SHAPS) for assessing the presence of anhedonia. In addition, open-ended questions were included in order to evaluate sociodemographic characteristics of the participants.
Beck Anxiety Inventory: To evaluate anxiety symptoms, the validated Spanish version of the BAI was adapted14. The psychometric properties of the instrument in the Chilean population have been evaluated with the sample of this study by the authors of this research (Cronbach's α=0.929; four-factor model fit indexes IFC=0.93, TLI=0.918, RMSEA=0.063, SRMR=0.041). The BAI is a useful tool to assess the physiological (somatic) and cognitive aspects of anxiety that a person may have experienced in the week before its application. The questionnaire consists of 21 questions, providing a range of scores between 0 and 63. Each item is scored from 0 to 3, with the score 0 corresponding to ‘Not at all’ 1 to ‘Mildly, but it didn’t bother me much’, 2 to ‘Moderately – it wasn’t pleasant at times’ and the score 3 to ‘Severely – it bothered me a lot’. According to the latest edition of the original manual, the study authors interpreted the BAI scores, which propose the cut-off points that define different levels of severity of anxiety symptoms. The cut-off points were 0–7 minimal anxiety, 8–15 mild anxiety, 16–25 moderate anxiety, and 26–63 severe anxiety15. These scores were extracted from the Spanish adaptation of the BAI.
Snaith–Hamilton Pleasure Scale: SHAPS is a rapid screening battery made for assessing the presence of anhedonia, namely the inability to experience pleasure. The Spanish-translated version of SHAPS was applied in the Mexican population16 with Alpha Cronbach’s α values of 0.77. The psychometric properties of the instrument in the Chilean population have been evaluated recently by the authors of this research (Cronbach's α=0.904; four-factor model fit indexes IFC=0.959; TLI=0.947; RMSEA=0.057; SRMR=0.034). This scale considers 14 sentences with a brief description of situations or pleasant sensations related to the last days and a scale of four possible answers among which the subject must indicate with an ‘X’ the one that best describes him/her: ‘Totally disagree’, ‘Disagree’, ‘Agree’, ‘Totally agree’. Any ‘Agree’ response is scored as 0 and any ‘Disagree’ response is scored as 1. The original scoring was used to investigate the proportion of participants that could be classified anhedonic (original SHAPS score >2)17,18.
Food frequency questionnaire: To evaluate food consumption, a previously validated food frequency questionnaire with closed-ended questions was applied19,20. A total of 25 experts participated in the expert judgement; the questionnaire was developed using the Delphi method. To assess the validity of the questionnaire used in this study, the Cronbach’s alpha was calculated, which was 0.77.
Diet quality was evaluated using a questionnaire consisting of 13 multiple-choice questions, specially designed to determine eating habits. The Food Quality Survey included two subscales: ‘Healthy eating habits’ and ‘Unhealthy eating habits’. The first subscale consisted of eight questions, with a minimum score of 1, an intermediate score of 3 and a maximum score of 5 for each question (Likert-type scale). The score indicated frequency of healthy habits and frequency of consumption of recommended food groups (fruits, vegetables, dairy products, eggs, meat, legumes, breakfast and bread). Each question was scored from ‘no consumption’ (1 point), ‘consumption is lower than recommended’ (3 points), to ‘suggested daily/weekly portions’ (5 points). This gave a score for the total of the answers on this subscale, which varied from 8 to 40 points (a higher value indicated better eating habits). The second subscale, ‘Unhealthy eating habits’, consisted of five questions, with a minimum score of 1, an intermediate score of 3 and a maximum score of 5 per question (Likert-type scale). The questions indicated foods or food groups identified as promoting chronic non-communicable diseases (pizza, fried foods, alcohol, pastries, sugary drinks), as well as the frequency of their consumption. Each question was scored from ‘inadequate eating habits’ (1 point) to ‘does not consume’ (3 or 5 points as appropriate). For unhealthy foods, the scores were reversed – ‘frequently consumes’ (1 point), ‘occasional consumption’ (3 points), ‘does not consume’ 5 points – giving a score for the total of the answers on this subscale, which varied from 5 to 25 points (a higher value indicated better eating habits). Finally, both scales were added up for the final score (13 to 65 points).
Statistical analysis
The statistical software Jamovi v1.6 (Jamovi Project; http://www.jamovi.org). To analyze the association between diet quality and anhedonia or anxiety in the rural context, a linear regression model was implemented. In the models, diet quality was included as a dependent variable and anhedonia and anxiety as independent variables. The model was adjusted by biological sex (male, female), age (years), level of education (primary/secondary, university), confinement (yes, no), availability of basic public services (some, all) and country (LRχ=65.51, df=18, p<0.001, R2=0.088). The analysis was performed using R (R Core Team; http://www.r-project.org) and RStudio (RStudio; http://www.rstudio.com). Models were fitted using the root mean square and figures plotted using ggplot221,22.
Ethics approval
The study followed the Declaration of Helsinki regarding work involving humans and agreed with the Singapore Statement on Research Integrity. The study was approved by the Scientific Ethics Committee of the Universidad de Las Americas, Chile, number 2020001, and was reviewed by committees of the participating countries.
Results
General characteristics of the sample
The sample included 708 people from rural areas in 11 Latin American countries, including Argentina, Chile, Colombia, Costa Rica, Ecuador, Guatemala, Mexico, Panama, Paraguay, Peru and Uruguay. Most participants were young, highly educated females (Table 1). More than half of the participants were working and were confined at the time of the survey (Table 1). About 80% of the households had all basic services including drinking water, electric lighting and gas supply (Table 1).
Table 1: General characteristics of the study sample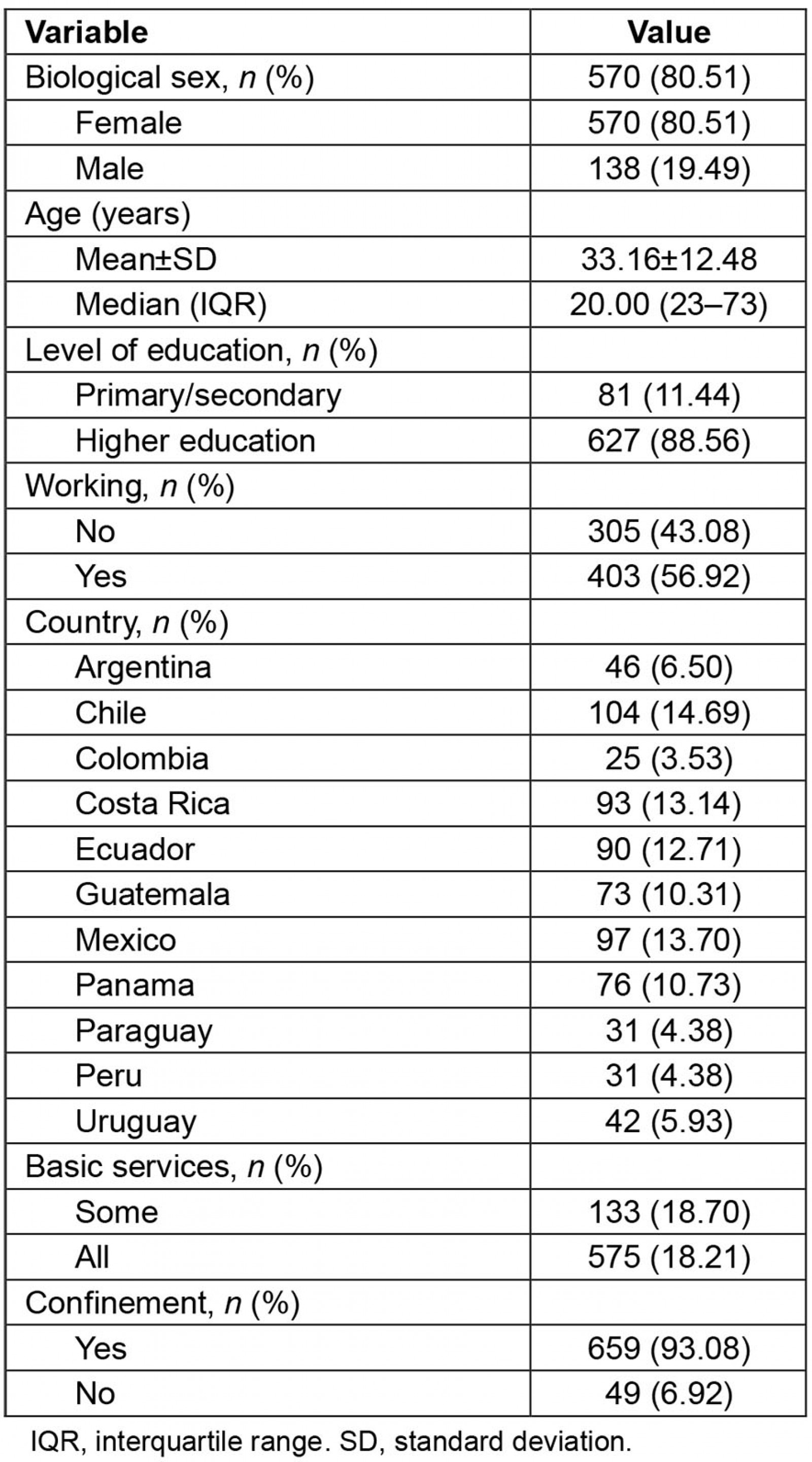
Diet quality, anhedonia and anxiety
In order to analyze the association between diet quality, anhedonia and anxiety in the rural context, the authors implemented a regression model with diet quality as a dependent variable. The model was adjusted by biological sex, age, level of education, confinement, availability of basic public services and country (see Methods). It was found that diet quality was inversely associated with anhedonia (F=11.98, p<0.001) and anxiety (F=9.11, p=0.003) (Table 2). The lower the score of diet quality, the higher the score of anhedonia; that is, anhedonia was related to a poorer diet quality (Fig1). Similarly, the lower the score of diet quality, the higher the score of anxiety; that is, anxiety was related to a poorer diet quality (Fig2).
Table 2: Diet quality, anhedonia and anxiety, based on rural Latin American sample (n=708), surveyed April–May 2020†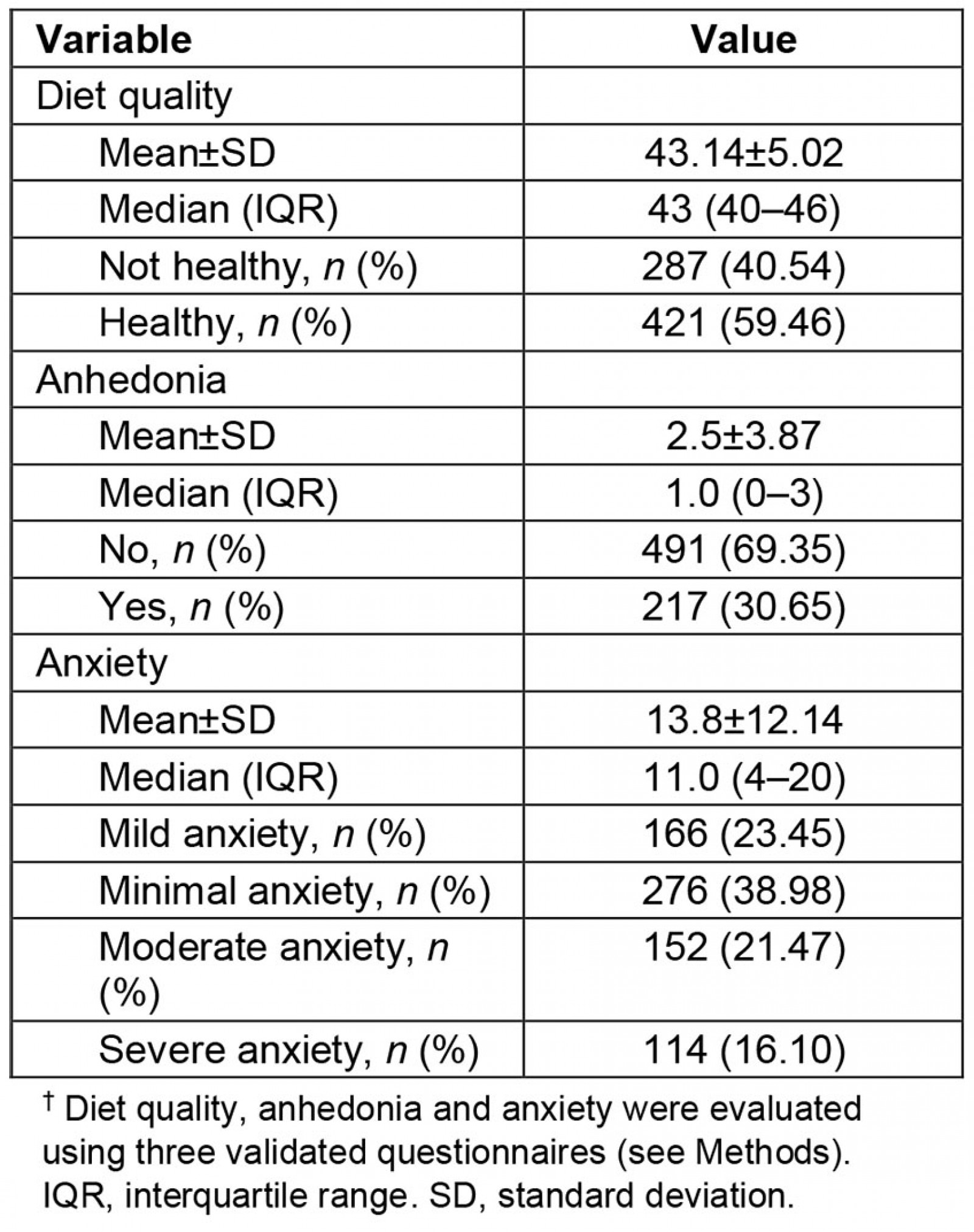
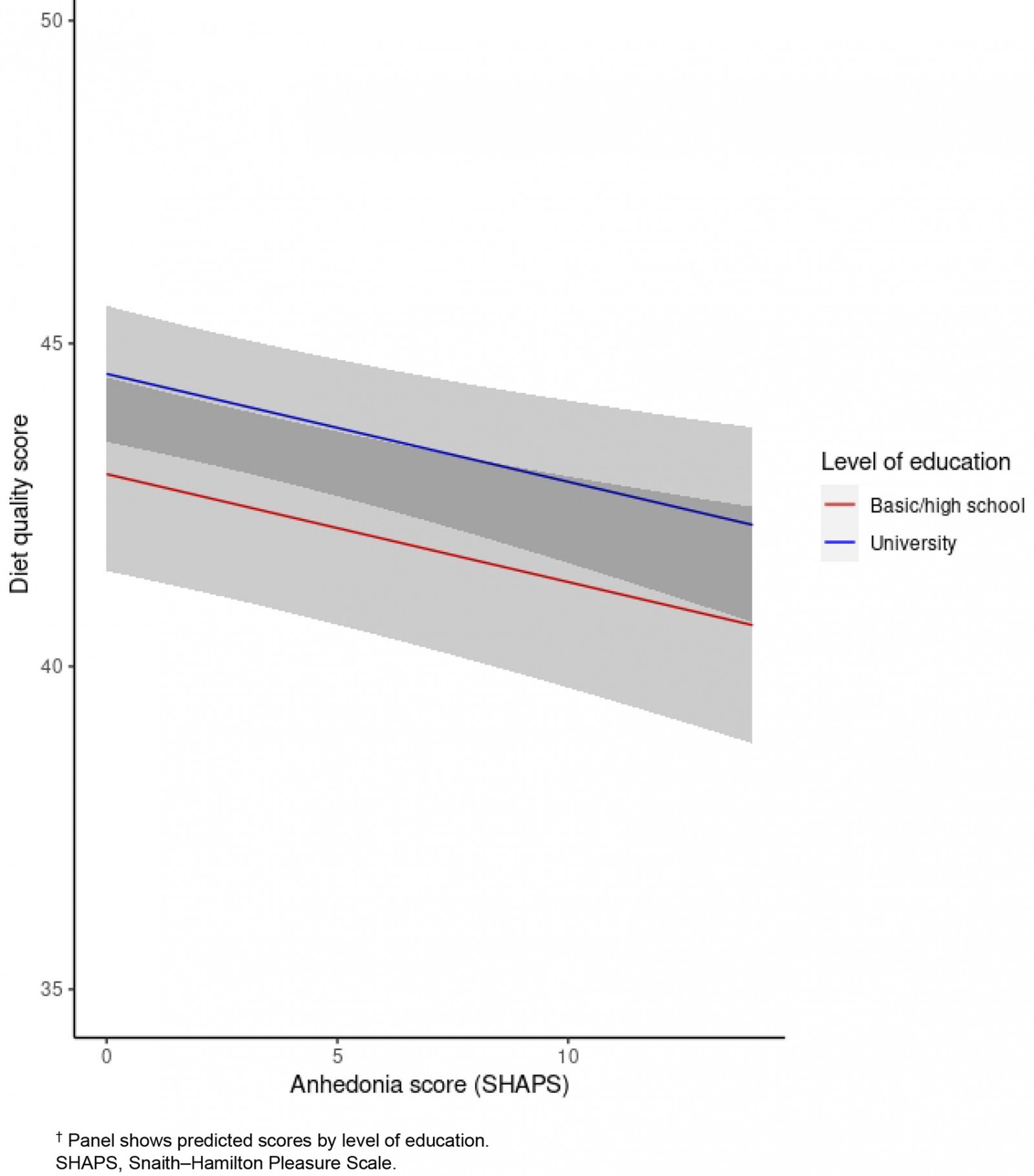 Figure 1: Association between diet quality and anhedonia, based on rural Latin American sample (n=708), surveyed April–May 2020.†
Figure 1: Association between diet quality and anhedonia, based on rural Latin American sample (n=708), surveyed April–May 2020.†
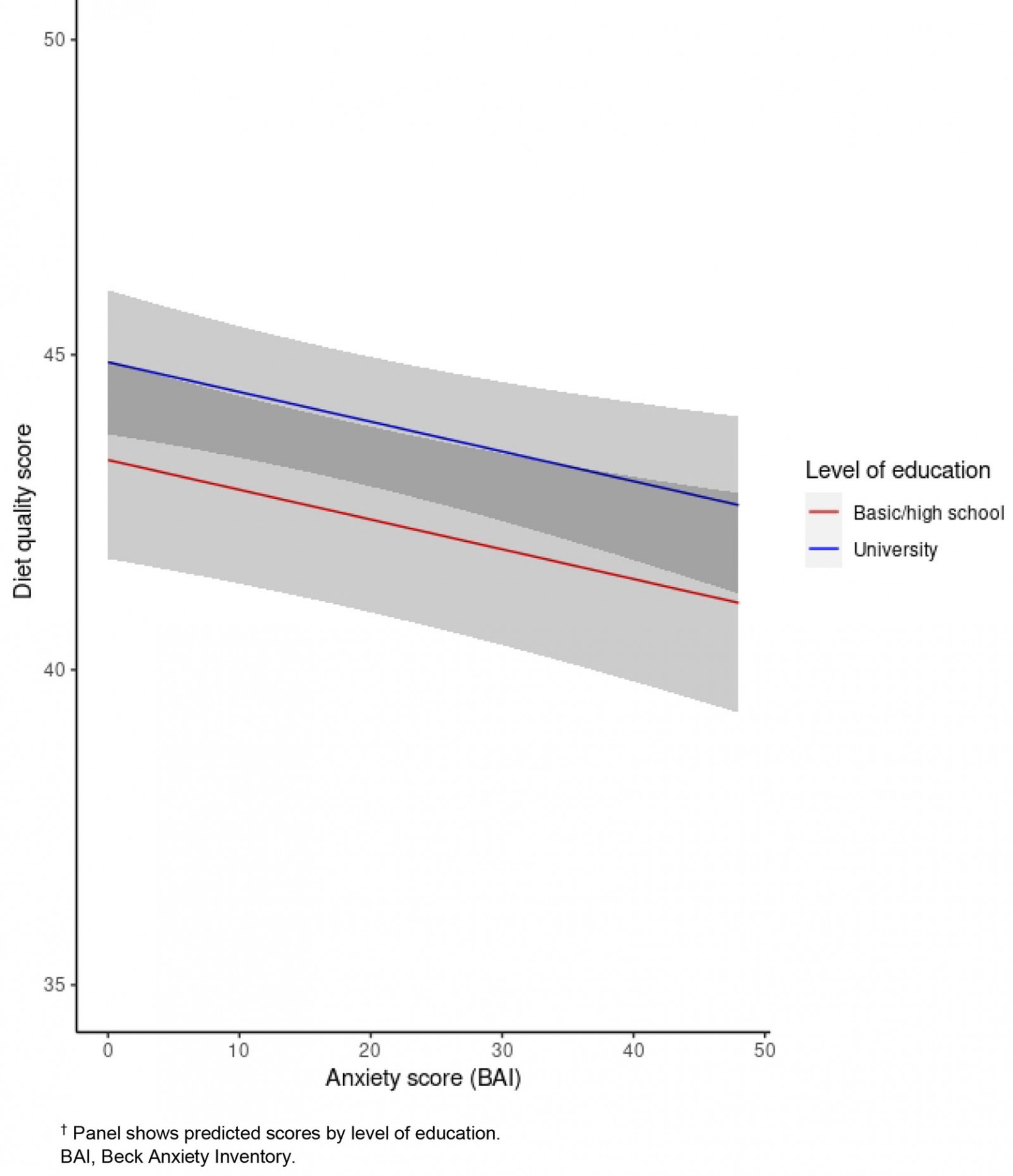 Figure 2: Association between diet quality and anxiety, based on rural Latin American sample (n=708), surveyed April–May 2020.†
Figure 2: Association between diet quality and anxiety, based on rural Latin American sample (n=708), surveyed April–May 2020.†
Diet quality and covariates
Diet quality was also associated with biological sex (F=4.75, p=0.030), level of education (F=7.00, p=0.008) and country (F=2.35, p=0.001). In this way, males and people with less education showed lower scores for diet quality than did females and highly educated people, respectively, suggesting that they have a poorer diet quality. Differences in diet quality by country are shown in Figure 3. By contrast, diet quality was not associated with age (F=0.57, p=0.451), work (F=0.68, p=0.410), type of quarantine (F=2.10, p=0.148) or no availability of public services (F=2.70, p=0.101).
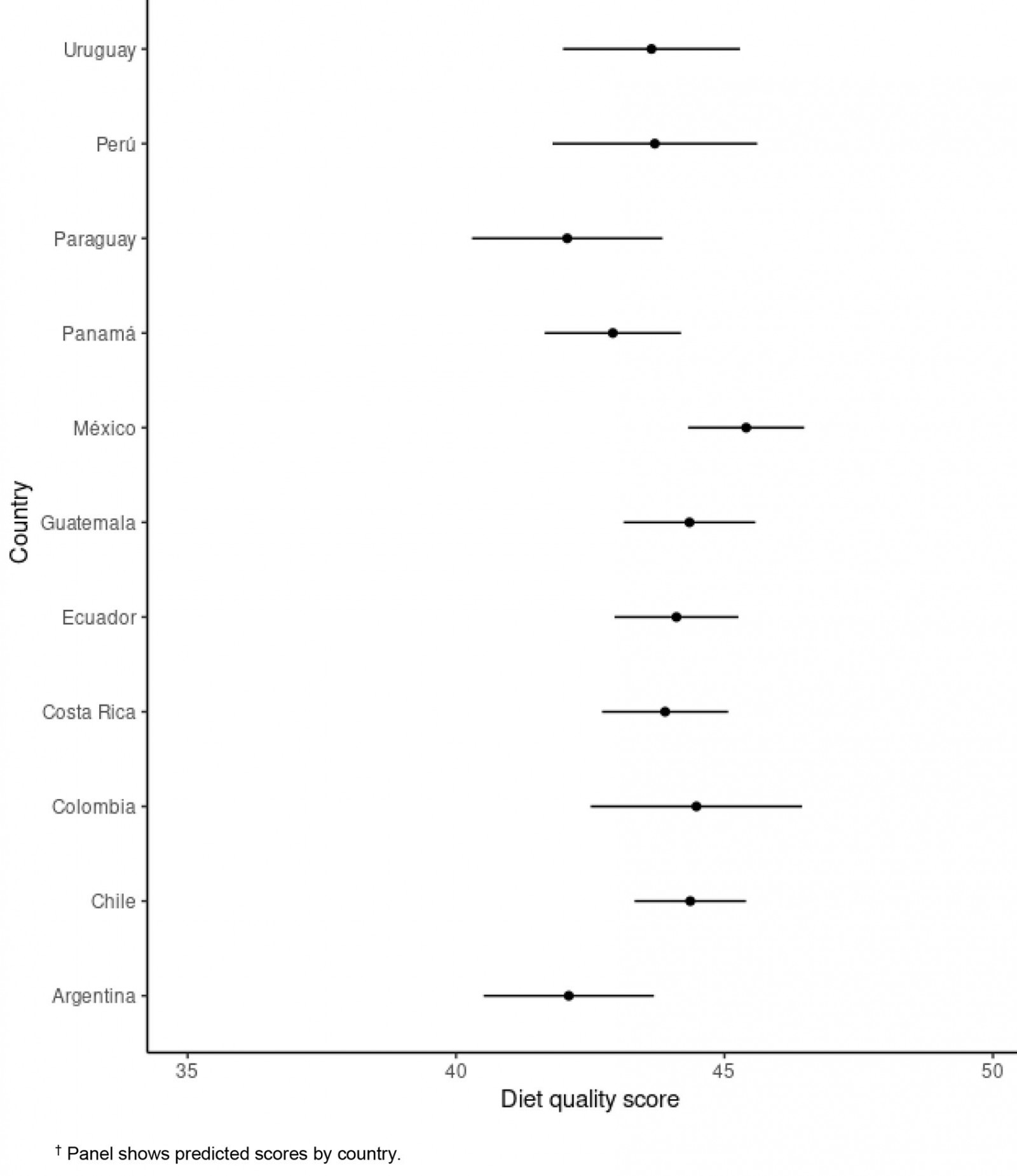 Figure 3: Association between diet quality and country, based on rural Latin American sample (n=708), surveyed April–May 2020.†
Figure 3: Association between diet quality and country, based on rural Latin American sample (n=708), surveyed April–May 2020.†
Discussion
At the time of writing, there were few studies addressing aspects related to diet and mental health among rural population. In this study, the main result shows that, among rural populations in Latin America, diet quality is associated with anxiety and anhedonia. In these populations, a lower diet quality is also associated with low level of education, and it was higher in men than in women.
In the context of the COVID-19 pandemic, actions taken in the field of public policies, such as confinement, are meant to protect individuals, especially the most susceptible ones, such as elderly people and those with chronic non-communicable diseases. These actions, although necessary, have negative implications for people, such as an increase in sedentary lifestyle, stress23 and the facilitation of unhealthy eating, leading to weight gain and favoring the occurrence of obesity-related non-communicable diseases. The effects of confinement on people living in rural areas were likely overshadowed, because official information from the governments or media is focused only on large cities.
In a study conducted among the Chilean population (n=1725) during the pandemic, in which the same surveys about anhedonia and anxiety were applied, significant correlations between the consumption of fried food and the perception of body weight gain were observed. In addition, anxiety was increased by the consumption of fried food24. Conversely, a study in a rural Italian population during the pandemic (n=359) showed a significant increase in the daily consumption of carbohydrates, all fresh vegetables, healthy vegetable oils, milk and yoghurts, alcoholic drinks, sugars and sweets, and coffee. The weekly consumption of lean meat, cured meats (other than ham), cheeses, eggs, nuts and mixed seed oils significantly increased, while the weekly intake of fish, mussels and legumes significantly decreased during lockdown; in addition, dietary quality index was reduced25. Another study, conducted in the USA and also focused on a rural population, showed that alcohol consumption increased among women with young children26,27.
It is likely that reduced access to healthy eating due to price rises, decreases in supply, lower incomes because of unemployment or job loss, and purchase restrictions28,29, may ultimately affect an adequate diet and favor the consumption of foods with a more satiating effect, such as bread, sugary drinks, baked goods and street food, which are low-cost, highly palatable and very affordable foods30. The authors have previously shown that there is high consumption of sugary drinks during a pandemic in an Ibero-American multicentric study. Among the factors associated are being male, having lower education and living in a rural area31.
These circumstances can lead to a Western-type diet that may promote obesity32, non-communicable diseases and cardiometabolic diseases33. Obesity is characterized by favoring the development of metabolic disorders and chronic low-grade systemic inflammation, which causes a pro-inflammatory microenvironment, further aggravating the production of cytokines and the risk of cytokine storm response during SARS-CoV2 sepsis. Furthermore, metabolic deregulation is closely related to an impaired immune system and an altered response to viral infection, which can lead to a greater susceptibility to infections, and greater duration and severity of disease34. Given these unfavorable conditions caused by obesity and its response to COVID-19, the policies and programs for promoting healthy eating and healthy lifestyles appear to be the best options.
Education level in the present study was an important predictor of food quality. Similar results have been found in other studies, as in the case of a prospective cohort study showing that a higher education level and favorable characteristics related to lifestyle, (including practicing physical activity and not smoking) predicted, at the beginning of the study, an increase in healthier dietetic patterns during 4 years of follow-up35. A cross-sectional observational study conducted with Brazilian adults showed that the lowest intake of some nutrients (calcium and vitamins A, C and D) was associated with a lower education level; the authors emphasized the promotion of healthy eating to counteract these deficiencies36.
It is important to note that reducing the consumption of food with pro-inflammatory properties, such as added sugars (sugary drinks and baked goods) and saturated fats (sausages/cured meats), and possibly increasing the consumption of food rich in unsaturated fatty acids with well-known anti-inflammatory properties, could represent a useful strategy to face this pandemic37. In a systematic review that assessed dietary intake in low- and middle-income countries, authors compared diet quality using socioeconomic level, which is strongly related to education level; it was found that people of high socioeconomic level were associated with greater consumption of fruits and/or vegetables, better diet quality and greater food diversity38. Among rural populations, 56% of this population worldwide do not have access to basic healthcare services39, supporting the present authors’ hypothesis of the emerging attention required by this group, both in Latin America and at the global level.
In addition, the pandemic is expected the increase of rural poverty and informal work, especially in low-income countries, even exceeding 90%. The lockdowns in rural areas, although probably not as strict as in urban areas, could restrict both work-related movements and the ability to return home, sometimes leaving people stranded and excluded from family support. Women in rural areas have been strongly affected because they are an important group of service workers and participate in informal jobs.
This study also found that women have a better quality of diet than men. Previous studies have observed variations in the dietary consumption of men and women and have been related to aspects of health such as weight change40 and cognitive function41. Other studies have reported greater problems with diet in women, but this has been done specifically in regards to the prevalence of food insecurity in these groups42,43. Therefore, men and women require differentiated attention in dietary recommendations and public care policies.
Among the weaknesses of this study, are that, because this was an online study, people who answered the instrument tended to be younger and with a higher level of education, and internet connectivity. Although people with less schooling had higher values of anxiety and anhedonia, these values did not reach significance for representing a reduced group. Finally, because this is a cross-sectional study, the authors cannot speak of causality, but only of association; therefore, it is recommended to conduct more studies on these topics.
Among the strengths of this study are the internationally validated surveys, allow comparison of results with those of other groups. Another strength is the number of survey responses for a rural population in Latin America – this study is one of the first of its kind. Finally, a higher proportion of women than men participated in the survey. This is probably because it was a survey that generated greater interest in women.
Conclusion
In this study, people with a lower level of education and lower diet quality in rural populations of Latin America indicated more anhedonia and anxiety during the COVID-19 pandemic, which will have consequences in the medium- to long term – particularly among women, who were the majority in this sample. It is necessary to conduct educational campaigns so that populations adopt healthy lifestyles during confinement.
Acknowledgements
We acknowledge Jorge Morales for his collaboration in the making of the figures.
References
You might also be interested in:
2012 - Potentials of a ten dollar pre-paid public health plan for rural health in Sub-Saharan Africa
2010 - Factors of primary care demand: a case study
2007 - How do we define 'rurality' in the teaching on medical demography?