




Introduction
Increases in life expectancy are not restricted to developed countries. Developing nations, such as Brazil, have entered a demographic transition phase. According to data from the Brazilian Institute of Geography and Statistics, Brazil has approximately 212 million inhabitants. Of these, 28 million are elderly and projections indicate that there will be 41.5 million in 20301.
With aging, a series of changes in cellular, tissue and systemic activity lead to physiological insufficiencies whose frequency and intensity lead to an increase in the demand for public health services. The greatest concern is the ability to offer preventive healthcare services to elderly people2. Most individuals in this population group undergo changes in the neuromuscular system, resulting in reduced muscle mass and strength, flexibility, resistance, joint mobility, coordination and balance3. The morbidity and mortality profile changes in an older population and contributes to a higher occurrence of chronic diseases, which are more prevalent among women4-6.
Although diseases and disabilities are not necessarily correlated with the aging process, chronic degenerative diseases have a higher incidence among the elderly. Thus, a significant number of people, despite living longer, have chronic conditions. Chronic non-communicable diseases are one of the biggest public health problems worldwide7. In Brazil, these diseases are prevalent in 70% of the elderly, causing a major impact on health. Hypertension, diabetes, osteoarthritis, neurodegenerative diseases, chronic lung diseases and cancer are the leading ones. Among the diseases that affect the osteoarticular system – musculoskeletal disorders with or without tissue damage – many of them cause chronic pain8, which negatively affects the health of the elderly9.
The International Association for the Study of Pain has defined chronic pain as an emotional, sensitive, uncomfortable experience lasting for more than 3 months. Its manifestation may be persistent or recurrent, and the typology of chronic pain can refer to both location and intensity. Chronic pain is a frequent complaint among the elderly, and it is one of the health problems that most interferes with performance and autonomy of basic daily activities10. It may be related to chronic pathological processes that persist for months or years, and pain is the main cause of functional limitation11.
The main influences on the use of and access to health services by elderly people with chronic pain are pain intensity, psychological suffering and socioeconomic determinants12. Vulnerable populations, such as low-income elderly people, can experience chronic pain for a long time without resolving the condition. The use of health services by individuals with chronic diseases, mostly elderly, is considerably higher than that observed among the general population, particularly regarding hospital admissions. Elderly people living in rural areas with multiple care needs are the ones who are most affected as they face significant barriers in accessing health services13,14. The Unified Health System (Sistema Único de Saúde, SUS) in Brazil faces challenges with regard to human, material, technological and healthcare alternative resources to deal with the specificities of an aging population15.
Thus, studies investigating the epidemiology of chronic pain in poorly studied socioeconomic and environmental contexts are of great importance. The aim of this study was to describe the sociodemographic profile and identify the prevalence of chronic back pain and associated factors in elderly people living in rural riverine areas in the state of Amazonas, Brazil.
Methods
Study design
This study analyzed data from a cross-sectional, home-based survey conducted in 2019 in 38 riverine rural areas along the left bank of the Negro River in the municipality of Manaus, Amazonas, Brazil.
Area and study population
The rural areas covered in the survey are only accessible by river. The most distant location surveyed was a 12-hour commute from Manaus using a regular form of transportation. The surveyed locations are assigned to a basic fluvial health unit of the Municipal Secretary of Health of Manaus, which operates up to the border between the municipalities of Manaus and Novo Airão. The service is itinerant and the fluvial health unit monthly trips last 10 days, with the team’s professionals remaining on board during this period. On the trip, the vessel stops at 13 locations throughout the territory, to assist the stopover location and surrounding areas. A large part of the population lives essentially from activities related to fishing, agriculture and plant extractivism.
Population and sample
Residents aged 60 years or older, who were selected in the households that constituted the sample, were included in the study. Stratified random sampling was carried out in rural riverine areas. A total of 287 out of 765 households were visited and 106 elderly people were interviewed in the households with residents in the age group of interest to the research. The random selection of one elderly person from each sex in the selected households corresponded to the second stage of the sample selection. The sample size calculation considered the likelihood of having an elderly person in the selected households as well as the estimated prevalence of 50% of the outcomes of interest and accuracy of 95%. Sample size was increased by 10% to compensate for possible losses or refusals to participate, and adjustment for the total number of elderly in the study territory (finite population, n=277). Information on the resident population in the territory was obtained from the Rural Health District of Manaus, which is responsible for the basic fluvial health unit in the area. The spatial distribution of the 85 households with elderly residents selected in the study is shown in Figure 1.
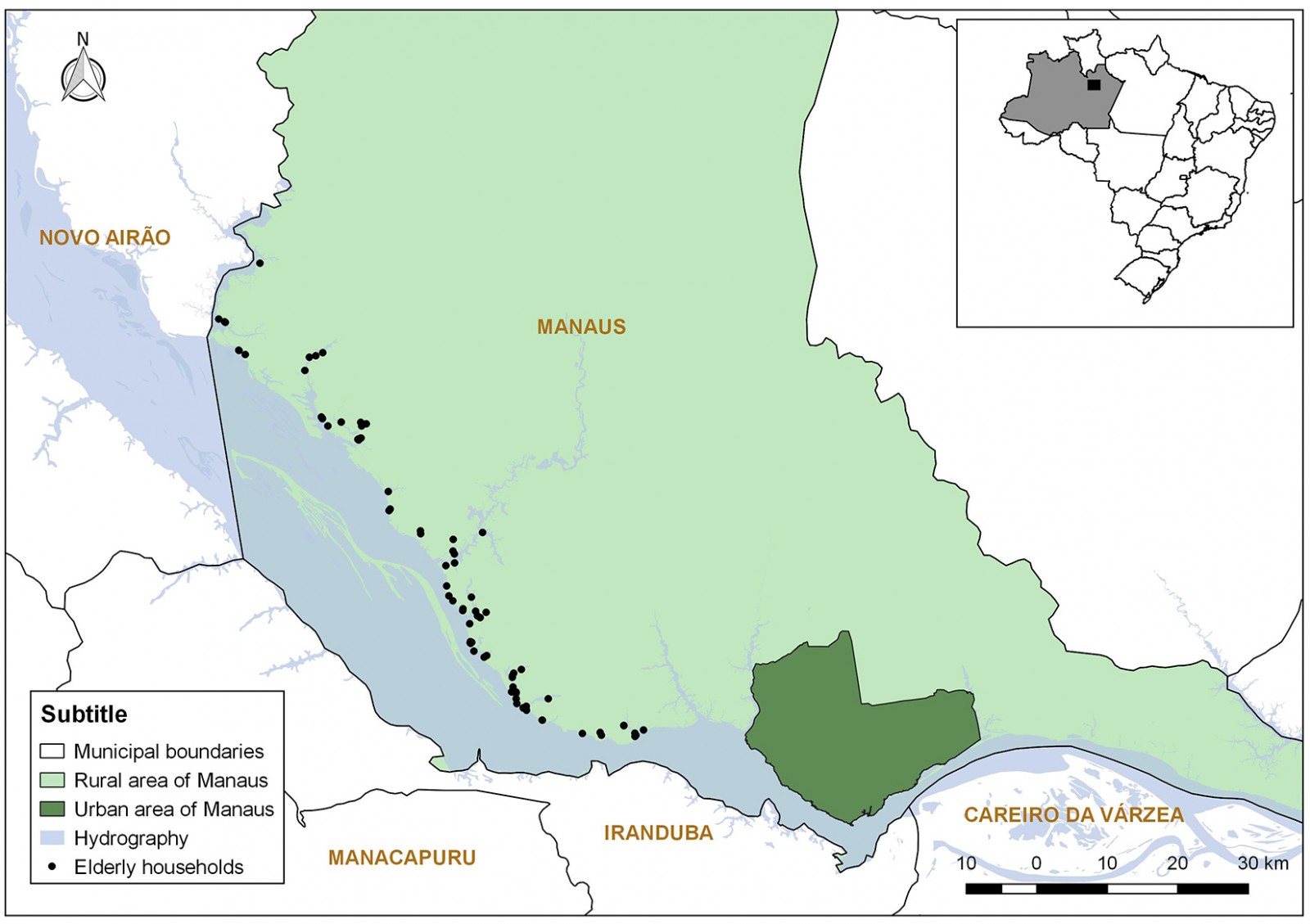 Figure 1: Households located along the left bank of the Rio Negro covered by the study, Manaus, Amazonas.
Figure 1: Households located along the left bank of the Rio Negro covered by the study, Manaus, Amazonas.
Data collection
The interviews were conducted on tablets and smartphones using the Research Electronic Data Capture (REDCap) to collect data. The selected elderly people answered a questionnaire with items related to their home, socioeconomic and demographic characteristics, aspects related to health, and the use and access to health services. The interviewers were previously trained on how to use the software application and were given information about the study methodology. A pilot study was carried out in two rural areas in Manaus that were not included in the survey.
The primary outcome of interest was assessed through the question ‘Do you have any chronic back problems, such as chronic back or neck pain, low back pain, sciatic pain, problems with the vertebrae or discs?’ (yes, no). The chronicity of pain was defined by the persistence of symptoms for more than 6 months10,16. If the answer was affirmative, the age at onset of symptoms and whether the elderly person took any action to solve the problem were evaluated.
The sociodemographic characteristics were age, sex, race/self-declared skin color, education, occupation and social benefits. The predominant material on the floor, walls and roof of the home was also evaluated, as well as the existence of electric energy, source of the water supply, sanitary sewerage and disposal of domestic waste.
The variables related to chronic conditions included the diagnosis of systemic arterial hypertension and diabetes mellitus, and the occurrence of cerebrovascular accident. For the elderly with any of these conditions, difficulty to perform daily activities and receive regular healthcare monitoring due to physical limitation were evaluated. The time since the last consultation with a medical professional, location of the service usually visited when ill and self-perception of general health were also assessed.
Data analysis
The data collected were transmitted from the mobile equipment to REDCap v3.4.1 (https://projectredcap.org) to check for possible inconsistencies and corrections of the records from the field diaries. After a critical analysis of the data and correction of inconsistencies, the dataset was exported from REDCap to the program Stata MP v15 (StataCorp; http://www.stata.com), and a descriptive analysis of the study variables was performed. Then, the association between the prevalence of chronic back pain was assessed and the independent variables using logistic regression was used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs). The variables with p≤0.10 in the bivariate analyses were selected for the multiple analysis, which estimated the measures of association adjusted for the outcome of interest. The significance level adopted for the multiple regression analysis was 0.05.
Ethics approval
The study was approved by the Human Research Ethics Committee of Fundação de Medicina Tropical Doutor Heitor Vieira Dourado (FMT-HVD; CAAE no. 57706316.9.0000.0005). After the participants had received information on the objectives, risks, and benefits of the research, they were invited to participate in the study and signed the free and informed consent form.
Results
A total of 1240 people lived in the 287 selected households. Of these households, 106 residents aged 60 years or older were selected. The mean age was 69.9 (standard deviation (SD)=8.2), ranging from 60.1 to 90.7 years. The average time that the families lived in the area was 33.1 years. In households with elderly people (n=85), the average number of residents per household was 3.2 and the average monthly household income was US$385.69 (A$521.06) (SD=208.32). Table 1 shows the household, socioeconomic and demographic characteristics of the elderly assessed.
Among the elderly interviewed, systemic arterial hypertension was the most prevalent chronic condition (50.0%). A total of 16.4% of the elderly reported a diagnosis of diabetes mellitus and 6.6% had already suffered a cerebrovascular accident. Of the 17 elderly with diabetes, 13 also had systemic arterial hypertension. Most elderly with hypertension and diabetes reported regularly attending a healthcare service due to their health status. Those who did not seek follow-up care reported that they did not think it was necessary. A total of 50.9% of the elderly with hypertension, 41.2% of the elderly with diabetes and 42.9% of the elderly with cerebrovascular accident reported having some limitation to perform their daily activities due to their disorder. The first healthcare service they seek is the one available in the community (57.6%), which includes health clinics and the fluvial mobile unit. Most of the elderly stated they had visited a doctor in the previous 12 months (85.8%) (Table 2).
The prevalence of any problem or chronic back pain among the elderly people interviewed was 57.5%, of which 38 elderly were men (63.3%) and 23 were women (50.0%). Most elderly reported they had not sought any treatment for their condition. On average, the back pain/problem started at the age of 43 years. Of those who sought some type of treatments (n=14; 22.9%), the following were the most reported: medication, walking or exercise, drinking homemade tea and ‘pulling’ (massaging the site of pain) along with physical activities. In the sample, 35 elderly (33.0%) reported having failed to perform any habitual activity for health reasons over the previous 2 weeks prior to the interview, and the main health reason that prevented daily activities was pain in the arms, hands, legs or feet (n=6; 17.1%). Table 3 shows the results related to chronic pain or reported back problem, self-perceived health and daily activity limitation due to health problems.
Table 4 shows the prevalence and the crude and adjusted ORs of chronic back pain or problem according to the categories of independent variables. The elderly who reported being civil servants or engaged in commercial or service activities showed a lower chance of the outcome when compared with those who performed agricultural activities (OR=0.1, 95%CI=0.0–0.9). A significant association was also found between worse self-perceived health and self-reported chronic back pain (OR=10.3, 95%CI=1.6-67.5).
Table 1: Household, socioeconomic, and demographic characteristics of the elderly, Rio Negro, Manaus, Brazil (n=106)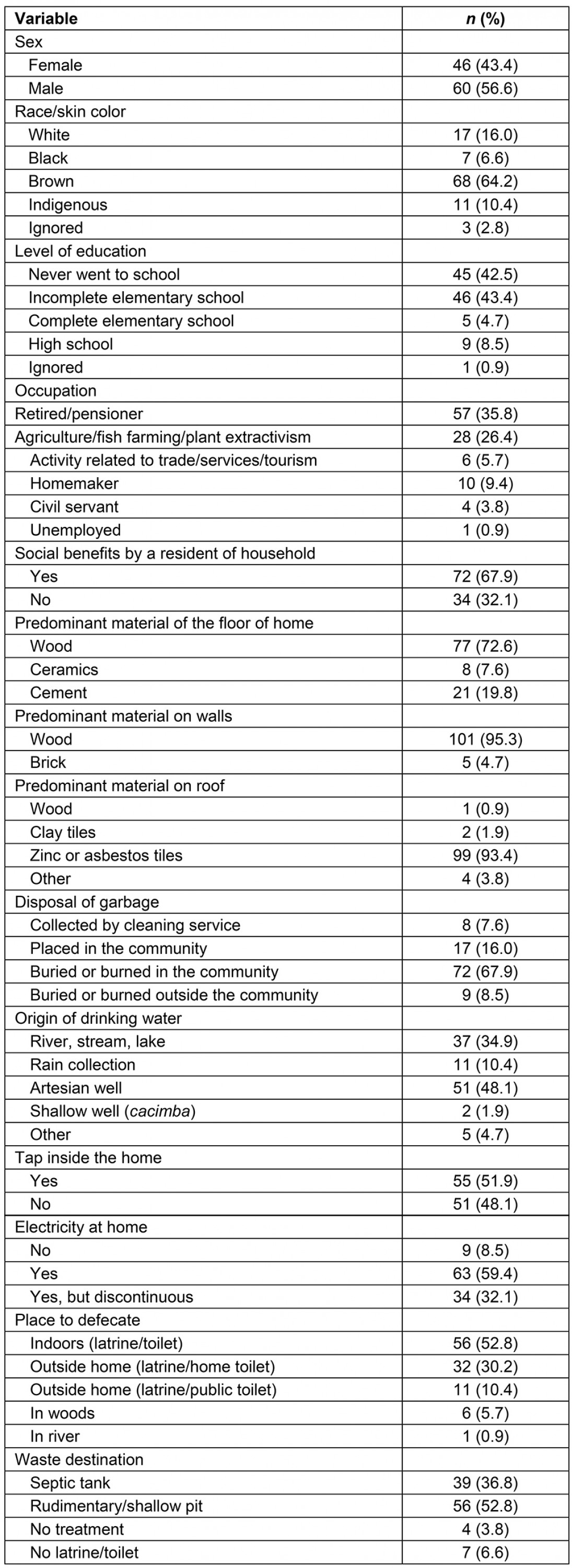
Table 2: Variables related to chronic conditions and use of health services by the elderly assessed, Rio Negro, Manaus, Brazil (n=106)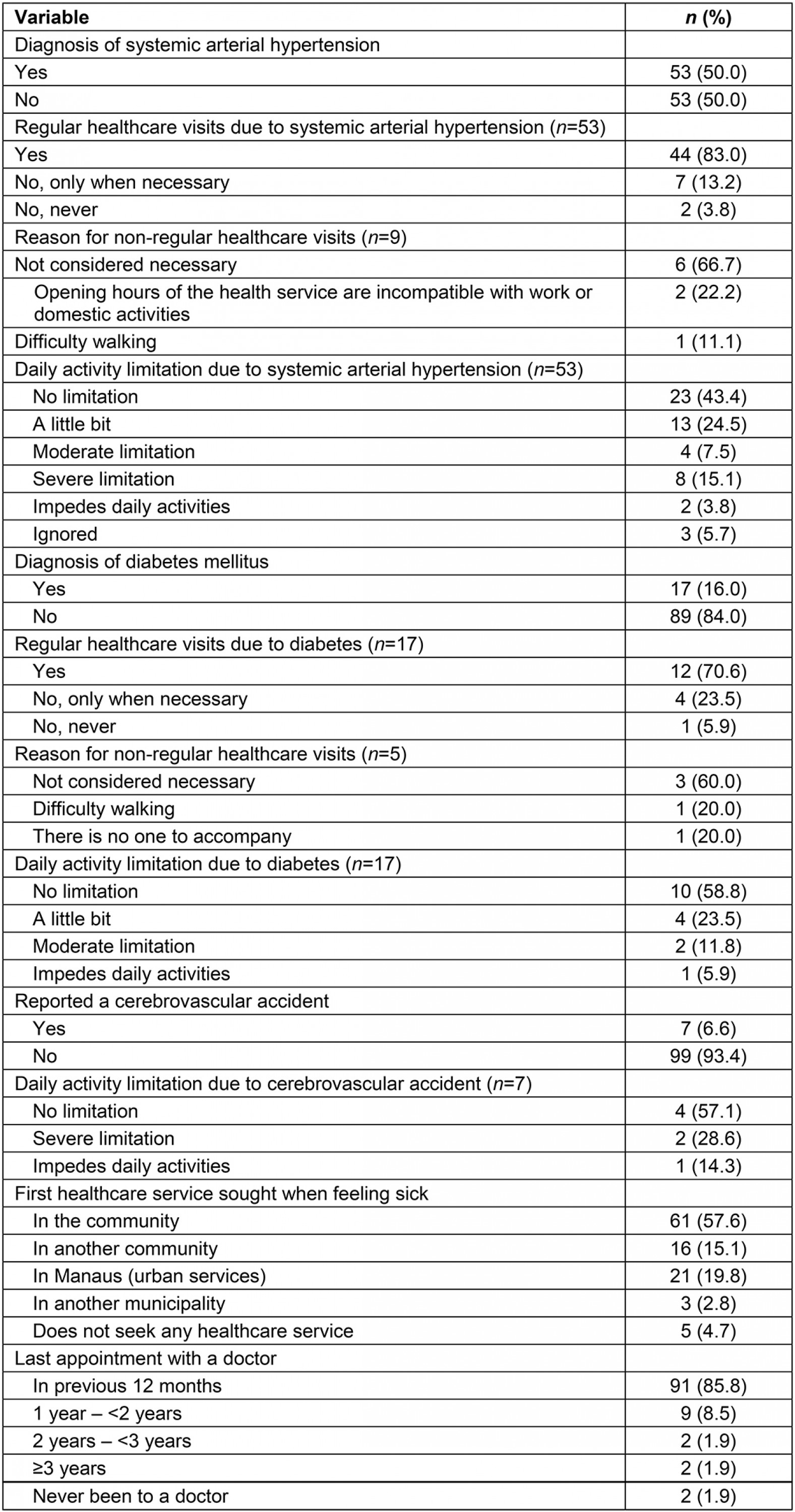
Table 3: Chronic back pain or problem, self-perceived health and daily activity limitation in the elderly assessed, Rio Negro, Manaus, Brazil (n=106)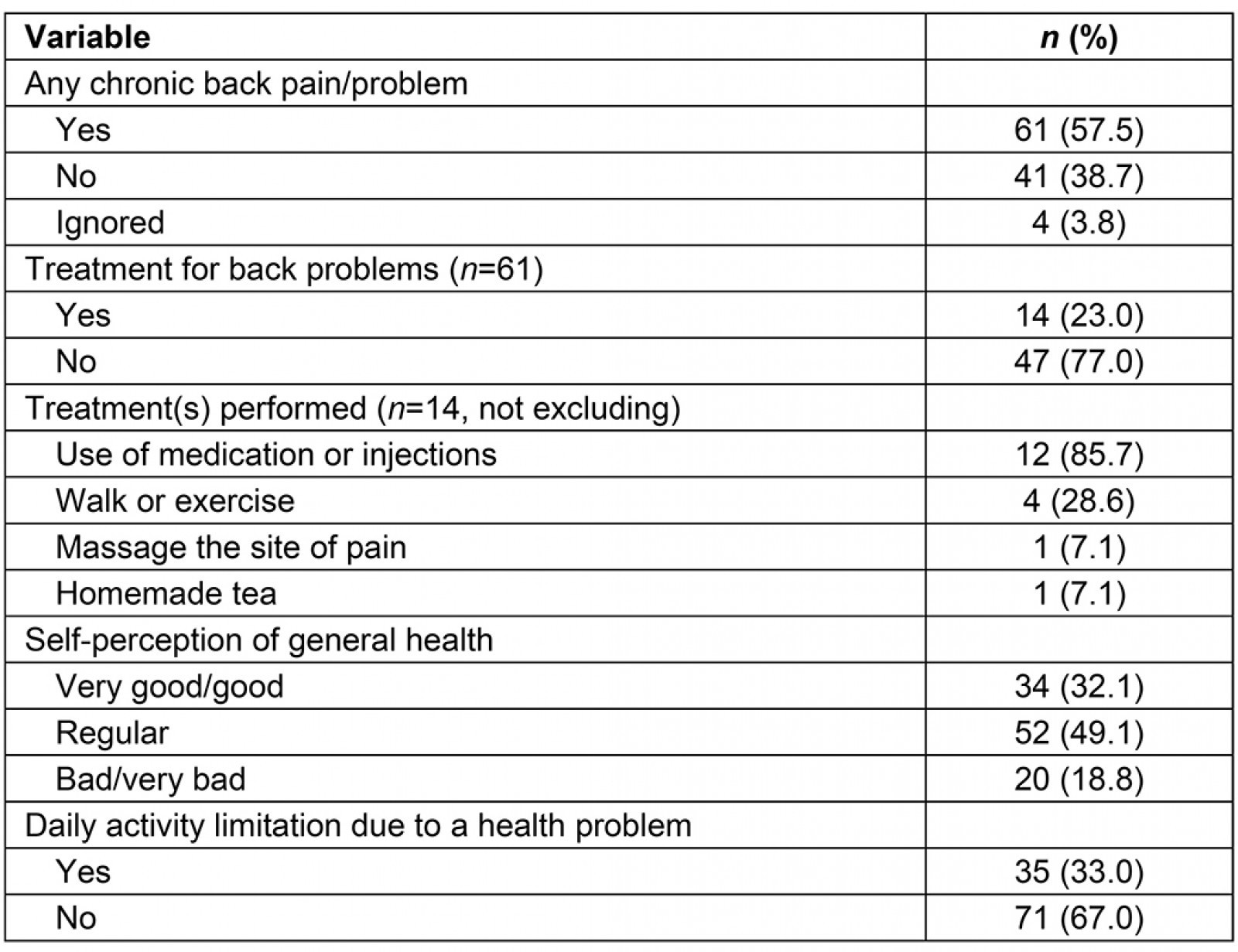
Table 4: Prevalence of chronic back pain or problem in the categories of independent variables and crude and adjusted odds ratios for the outcome, Rio Negro, Manaus, Brazil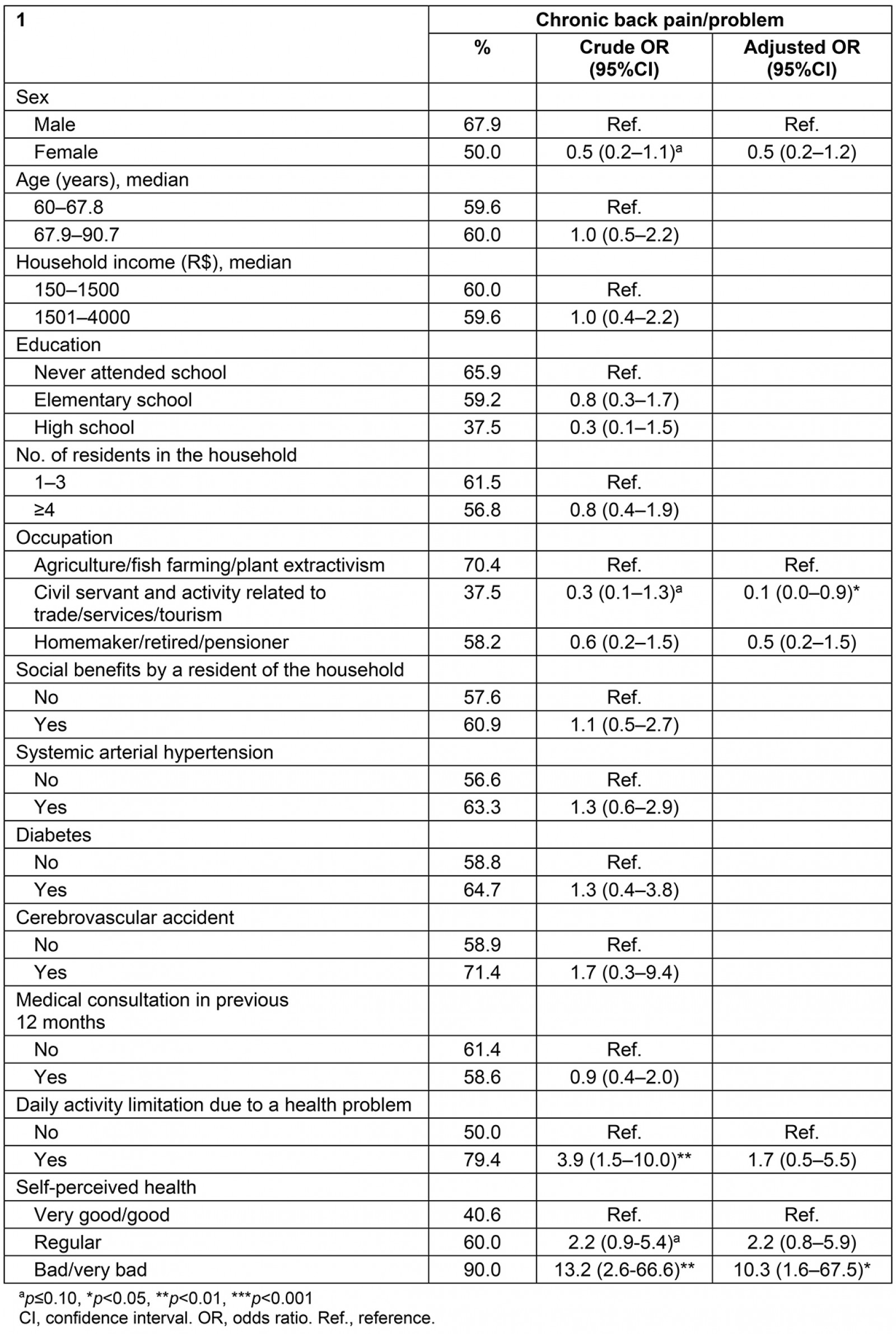
Discussion
In the present study, chronic back pain was an extremely prevalent condition in elderly people living in rural riverine areas. The findings also revealed limited access to treatments for the problem as well as usually being restricted to accessing drug interventions. Worse self-perceived health and agricultural activities were associated with the outcome assessed.
Estimates from a national home-based survey conducted in Brazil in 2013 showed that, in adults, the prevalence of chronic back pain increases with advancing age, having been reported by 25.5% (males) and 31.3% (females) over the age of 65 years17. A higher prevalence was also identified in rural areas of the country, but the difference was significant only among male adults17. A systematic review of chronic low back pain in the elderly identified a high occurrence of the outcome. However, the review found great variability among the studies included (21–75%) as the outcome depended on the evaluation criteria and the characteristics of the study site and population. The review also reported an association between low back pain and impaired functional capacity and dependence on help performing daily activities18. In a French population-based survey, chronic low back pain was associated with poor health-related quality of life for adults and the elderly. The authors also found a higher prevalence in rural areas (41.6%)19.
The organizational characteristics of the healthcare services offered to populations who reside in socially vulnerable and difficult geographic areas make it difficult to change the healthcare model aimed at spontaneous demand and to mitigate social and health inequalities faced by the elderly20. The low percentage of individuals with chronic pain who have undergone treatment represent less than half of that found in a national survey21. This same study showed that individuals with better socioeconomic conditions were more likely to undergo some type of treatment. Drug treatment was also the most frequent type of intervention, and this practice was more common among the most vulnerable groups, that is, those with low education, from a lower social stratum, who reside in rural areas and in the North, Northeast and Midwest regions. On the other hand, physical exercise or physiotherapy, the second most frequent intervention, was greater among the most socially favored people21.
A continuous rehabilitation process, involving a multidisciplinary approach to chronic back problems, can be more effective in reducing functional limitations and disabilities22. Thus, healthcare services should be organized, minimize social and individual impacts, and reduce public health costs. For chronic, predictable conditions, such as diabetes and hypertension, healthcare services can provide regular care, which is not the case for chronic back pain. Briggs et al23 identified that factors such as poor access to information and services, inadequate knowledge and skills among local practitioners, feelings of isolation and frustration, psychological burden and competing lifestyle demands are barriers to adopting regular self-management practices in rural contexts. Considering geographic accessibility and the availability of services in riverine rural areas, community-based self-management programs could be feasible and contribute to improve this situation24,25. The occurrence of the disorder becomes more frequent with advancing age17,26, suggesting that timely interventions should be applied to mitigate the evolution of chronic pain. An older population with a poor quality of life tends to demand more from healthcare systems, resulting in more expensive, specialized and permanent services27.
Several studies have shown a higher prevalence of chronic back pain in the most disadvantaged groups3,7,18,19,21,28,29. Although no association was found between individual socioeconomic factors and the occurrence of the outcome in the present study, the high prevalence may also reflect a contextual characteristic of vulnerability to which the study population is homogeneously exposed. The socioeconomic characteristics of the elderly assessed reveal the unfavorable living conditions of the rural riverine population who could, therefore, benefit from health promotion programs30. The socioeconomic vulnerability of the study population also reaffirms the importance of universal access to comprehensive and effective health care. The high prevalence of the elderly diagnosed with chronic diseases who have low education and low income, and who reported pain and perceived their health as regular, bad, or very bad, reinforces the importance of implementing programs aimed at chronic pain.
The elderly who performed agricultural activities or plant extractivism were more likely to report chronic pain. Occupational aspects have been reported in the literature as associated with this outcome, including heavy activities both at work and at home17. In the riverine rural environment, men and women are exposed to unhealthy work activities at an early age, which certainly contributes to the high prevalence observed in both sexes. Other studies have found a higher prevalence of chronic back pain in women18,19,31, which was not observed in this population. These occupational issues must also be addressed by public healthcare interventions.
Chronic back pain has several impacts on individual and collective health. Saes-Silva et al31 argued that if it were possible to eliminate this condition in the studied population, outcomes such as poor health perception, low quality of life and prevalence of depressive symptoms could be reduced by 25%. Other authors have reported associations of the outcome with poorer self-perceived health, disability and psychiatric morbidity3,17,32-34. Rodrigues et al35 also reported worse performance of the elderly with chronic low back pain on functional tests. Even if it does not completely disable the performance of daily activities, pain can partially or temporarily affect individuals, sometimes on a recurring basis35. The findings of the study show that the elderly who perceived their health as bad or very bad were 10.3 times more likely to have reported chronic back pain, suggesting that this impact also affects the rural riverine population.
It should be noted that the study was carried out with an elderly population living in a rural riverine area, that is, a socioeconomically vulnerable population that faces several difficulties to access services20. Self-reported measures can also vary among social groups due to different references when assessing their relative wellbeing or even differences in the interpretation of research questions36. The outcome could also have been measured in different ways, which could have influenced the results found. Therefore, generalizations of the findings should be made with caution. Even so, the study findings can be useful for the other fluvial health teams existing in the vast territory of the Amazon and Pantanal in Brazil, and for territories with similar geographic and social characteristics, including hard-to-reach rural areas in developing countries. Considering the cross-sectional design of the study, the causal inferences based on the association measures must also be interpreted with caution.
Conclusion
Based on the findings of the study, the high prevalence of chronic back pain or problem in rural riverine elderly people with limited access to treatment reveals that this condition is an important public health problem, as it impacts the performance of daily activities as well as the quality of life of the individuals affected. The vulnerability of the study population reaffirms the need for an organized public healthcare system, particularly primary health care, so that actions and strategies have an impact on social determinants and associated factors in a manner consistent with the living conditions of this population. Thus, proposing alternatives for more effective interventions, including preventive measures, multidisciplinary pain programs and community-based self-management programs, can minimize the individual and collective impact of chronic back pain as well as reduce financial and social costs.
References
You might also be interested in:
2022 - COVID-19 fosters social accountability in medical education