



Introduction
The COVID-19 pandemic began in March 2020, causing major disruptions to social activities, education, employment, and healthcare delivery1-3. Misinformation (unintentionally false information) and disinformation (deliberately misleading information) about COVID-19 were widespread4-6. For example, misinformation about hydroxychloroquine, an antimalarial drug, effectively treating COVID-19 contributed to public uncertainty about the pandemic and highlighted the importance of health literacy7. The influx of both inaccurate and accurate COVID-19 information was labeled as an ‘infodemic’8.
To be prepared for future infodemics, the role of health literacy with impacts brought about through the COVID-19 pandemic must be better understood9. Health literacy is the ability to access, understand, and use health information and services10. An individual’s health literacy level is often determined from their performance on health literacy assessments, where lower scores indicate limited health literacy and higher scores indicate adequate health literacy10. Limited health literacy is associated with poor overall health, while adequate health literacy is correlated with health and wellbeing11. An estimated 80 million adults (36%) in the US have limited health literacy, and limited health literacy is overrepresented in individuals who have lower socioeconomic status and/or are Black, Indigenous, and people of color (BIPOC)11,12.
Associations of health literacy with COVID-19 knowledge13, beliefs14, and behaviors such as vaccine hesitancy15 or refusal16 have recently been explored. Overall, these studies show that adequate health literacy is associated with greater knowledge of COVID-19 and engagement in preventive health behaviors (eg COVID-19 vaccination). Other factors, such as health consciousness17 and political ideology, may also play a role in COVID-19 beliefs and related behaviors14. This prior work contributed to this study’s conceptual framework linking health literacy to COVID-19 pandemic impacts at both the individual and household levels. We inferred that COVID-19 pandemic impacts would be experienced on both individual and household levels, but that these impacts would be most frequently identified at the individual level. According to past research, COVID-19 awareness and beliefs contributing to COVID-19 pandemic behaviors including immunization were thought to be more strongly associated with adequate versus limited health literacy. In turn, adequate versus limited health literacy, by way of COVID-19 awareness, beliefs, and behaviors, was thought to be associated with fewer individual and household adverse COVID-19 pandemic impacts and more positive COVID-19 pandemic impacts.
Still, a dearth of published work has examined associations of health literacy with negative and positive impacts resulting from the COVID-19 pandemic. Particularly in more rural areas with culturally diverse individuals, including Indigenous communities, little research has been conducted to better understand the relationship of health literacy with various impacts from the COVID-19 pandemic. Northern Arizona is home to Coconino County, the second-largest county in the contiguous US. Within the county, tribal lands (39.1%) and forest service (27.2%) make up much of its unique geography. Due to the rural nature of many of these inhabited areas, limited access to health facilities, grocery stores, and to reliable internet, further exacerbated adverse COVID-19 pandemic impacts for Northern Arizona residents18.
Because health literacy is a modifiable determinant of health, it is essential for future preparedness and response efforts to better understand how health literacy was related to COVID-19 pandemic impacts. This study sought to examine associations of health literacy with impacts from the COVID-19 pandemic among a diverse sample of adults in Northern Arizona. Based on past research and our conceptual framework12-17, we hypothesized that individuals with limited rather than adequate health literacy would experience more significant adverse impacts from the COVID-19 pandemic, with a greater likelihood of individual rather than household impacts.
Methods
Design
This cross-sectional survey was part of a larger randomized crossover trial19. Data were collected from June 2020 to August 2021.
Instruments
The survey’s questionnaire included measures of participant demographic and health characteristics, health literacy, and COVID-19 pandemic impacts.
Measures of participant demographic characteristics
To assess participant demographic characteristics, items were adapted from the 2020 National Health Interview Survey on age, biological sex, Hispanic ethnicity, race, health insurance coverage, marital status, and employment20. Additional questionnaire items on health status and quality of life from the 36-item Short Form Health Survey were included21.
Health literacy assessment
The Newest Vital Sign is a validated six-question tool that utilizes an ice cream nutrition label, and it is read aloud by an interviewer to assess a participant’s health literacy and numeracy skills21,22. Correct responses are scored with one point, and incorrect responses score a zero. Adequate health literacy is determined by a total score of four to six, while anything below indicates limited health literacy. A total score of zero or one indicates likely limited health literacy, and a total score of two or three indicates possible limited health literacy23.
COVID-19 pandemic impacts measure
The Epidemic–Pandemic Impacts Inventory (EPII) was developed to learn more about the impact of the COVID-19 pandemic and future epidemics and pandemics on an array of personal and family life domains24. A total of 92 items are included in the EPII. There are nine categories of negative impacts within the EPII: work and employment (11 items), education and training (2 items), home life (13 items), social activities (10 items), economic (5 items), emotional health and wellbeing (8 items), physical health problems (8 items), physical distancing and quarantine (8 items), and infection history (8 items). There are also 19 positive change items within the EPII. The following question stem preceded all the EPII items: ‘Since the coronavirus disease pandemic began, what has changed for you or your family?’ Each question within these categories allowed participants to answer ‘yes’ for themselves and/or someone else in their home (ie another person or people), ‘no’, or ‘does not apply’ to them or another person in the home. No psychometric properties or optimal scoring procedures were available for the EPII when this study occurred. Because the EPII does include one domain on positive change impacts, we separated this subdomain with 19 items in determining and analyzing the total number of adverse COVID-19 pandemic impacts. For descriptive purposes, we did however examine the 19 positive change subdomain items. Individual items are shown in Figures 1a–d.
Recruitment
Patients were randomly sampled based on the following criteria: (1) aged 18 years or older, and (2) had one or more visit(s) at either the Native Americans for Community Action Family Health and Behavioral Health Center or the North Country HealthCare Flagstaff (4th Street) clinic in Northern Arizona within the past 12 months of the sample being drawn. Recruitment initially occurred by mail, with an invitation letter containing study information. Patients at one of the federally qualified health centers were also contacted by telephone 1–4 weeks after the recruitment letters were sent if they had not already contacted the study team about participating. Some individuals were recruited through word of mouth. Eligibility based on inclusion criteria was confirmed by the research team prior to individuals’ participation. All individuals enrolled provided verbal informed consent.
Participants
There were 119 participants in this study: 19.3% had limited health literacy, and 80.7% had adequate health literacy. The average age of participants was approximately 54 years, and 56% were female. Nearly 23% of participants identified as American Indian or Alaska Native, and 73% identified as White. About 8% of participants identified as Hispanic, Latino, or Spanish. Slightly more than half of the participants (51.3%) were not employed, and 52% had public health insurance or no health insurance. Only two participants reported not having health insurance. Approximately 47% of participants were married, and 31% had children aged less than 18 years. Most participants (63%) rated their overall health as excellent or very good, and most participants (84%) were recruited from one of the two federally qualified health centers involved with this study. Table 1 displays participant characteristics.
Table 1: Participant demographics (N=119)†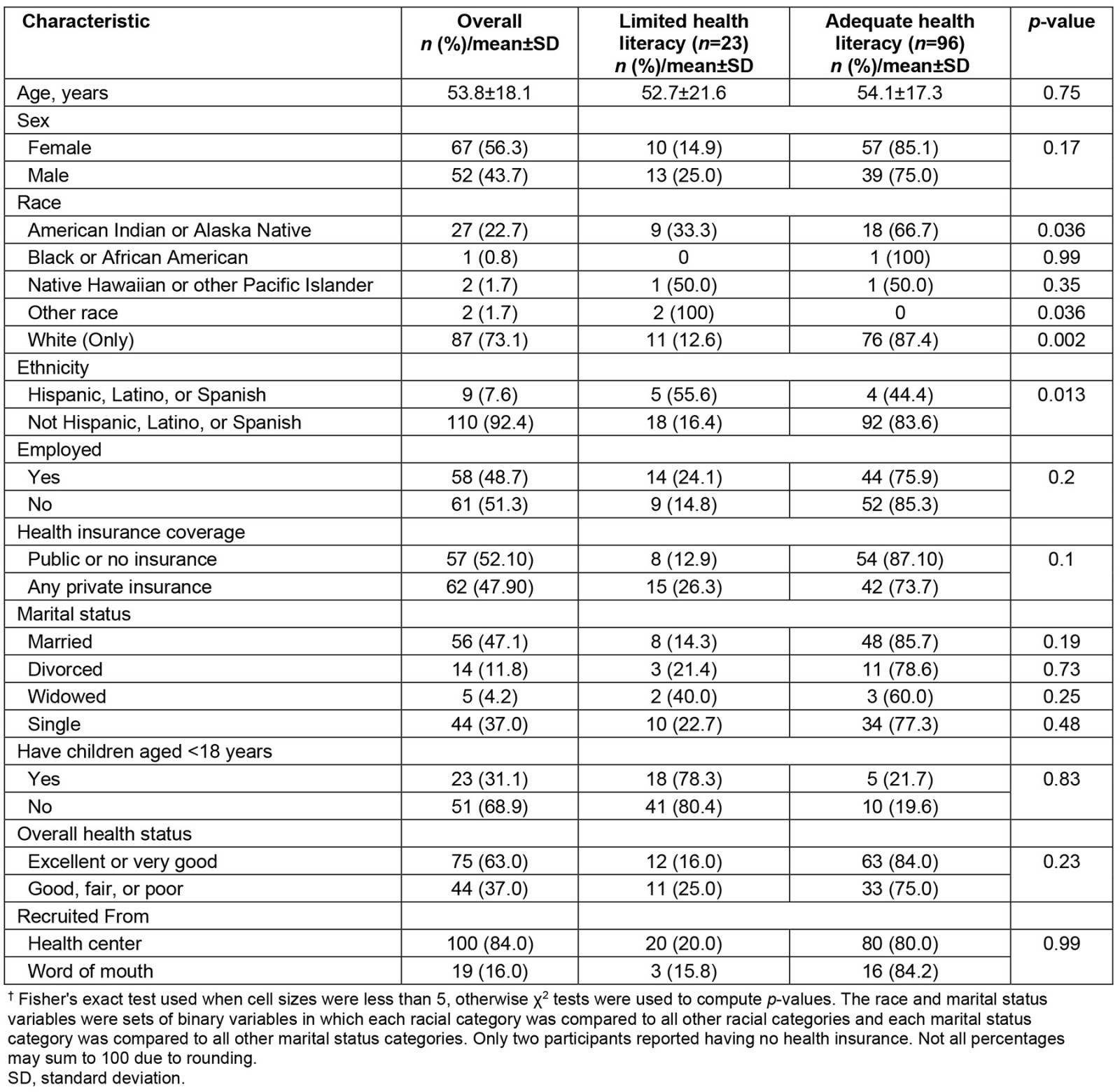
Procedure
The interviewer-administered survey was conducted via telephone or videoconference, depending on participant preference. Data were collected and managed using REDCap (Research Computerized Data Capture) tools hosted at the first author’s institution25. All research team members underwent training in administering the survey and collecting data in REDCap. Each participant received a $20 payment.
Analysis
Exploratory data analyses were initially performed by computing descriptive statistics such as means, standard deviations, frequencies, and relative frequencies to determine the distributional properties for all variables of interest and to characterize the sample. We created charts to visualize the frequency of the 73 adverse and 19 positive change COVID-19 impacts for participants individually and their households. Bivariate statistics including cross-tabulated proportions and means were computed to determine differences in participant demographic characteristics by health literacy level (ie limited versus adequate health literacy). Chi-squared or Fisher’s exact tests were used, as appropriate, for categorical variables. The total mean number of individual and household COVID-19 impacts reported was compared according to health literacy level using a Wilcoxon rank-sum test, given the skewness and kurtosis of the individual and household impact variables’ distributions26. We further examined differences in each of the 10 COVID-19 pandemic impacts areas (eg work and employment, home life) for individuals and households by health literacy level using the same approach insofar as a Wilcoxon rank-sum test was used to determine statistical significance when skewness was greater than 3 or less than –3 and kurtosis was greater than 7 or less than –7. Because the individual and household impacts variables were count variables and their conditional variances exceeded their means, two negative binomial regression models were fit. The independent variable of interest in these models was health literacy level (adequate versus limited); however, we additionally included several covariates that had statistically significant or marginally significant associations (p<0.20) with health literacy level including biological sex, health insurance status, and race and ethnicity. (Due to small cell sizes, categories were combined as follows: White and non-Hispanic; Hispanic, Latino, or Spanish; or American Indian/Alaska Native, Black/African American, Native Hawaiian/Pacific Islander, or other race.) We conducted sensitivity analysis based on our bivariate analysis results to further examine the multivariable associations of limited versus adequate health literacy with each of the three household COVID-19 impact domains (social, emotional, infection), adjusting for demographic factors using negative binomial regression models. All statistical tests were two-tailed, and an alpha level of 0.05 was used to determine statistical significance. Data were analyzed in Stata v17 (StataCorp; https:/www.stata.com).
Ethics approval
This study was granted approval by the Northern Arizona University Institutional Review Board (Protocol # 156183).
Results
Participant demographic characteristics and health literacy level
Participants who identified as American Indian or Alaska Native were significantly less likely to have adequate health literacy than those who identified as White only (66.7% v 87.4%, p=0.036). Participants who identified as Hispanic, Latino, or Spanish were also less likely than non-Hispanic participants to have adequate health literacy (44.4% v 83.6%, p=0.013). No other demographic characteristics were found to have statistically significant associations with health literacy (Table 1).
Frequency of COVID-19 pandemic impacts
On average, participants experienced an average of 14 impacts themselves (standard deviation 6.8, median 14, range 1–39, interquartile range 9–18), and their household experienced an average of one impact (standard deviation 3.8, median 0, range 0–25, interquartile range 0–23) of the 73 impacts measured (Table 2). The most frequently experienced COVID-19 impacts for individuals were in the domains of emotional health and wellbeing, social activities, and physical health problems. Participants reported the following individual impacts most frequently: spending more time on screens and devices (emotional health and wellbeing domain, 76%); having family celebrations canceled or restricted (social activities domain, 74%); having travel plans or vacations canceled (social activities domain, 71%); being separated from family or close friends (social activities domain, 68%); being unable to participate in social clubs, sports teams, or volunteer activities (social activities domain, 68%); being unable to do enjoyable activities or hobbies (social activities domain, 68%); and spending more time sitting down or being sedentary (physical health problems domain, 67%). The following COVID-19 impacts were not reported by any participants: becoming homeless, having an increase in physical conflict with a spouse, having an increase in physical conflict with other adults in the household, and having someone in the home who died of COVID-19. Impacts for the household generally followed a similar pattern but were reported far less frequently than the individual impacts experienced by participants. Figures 1a–d display the frequencies of COVID-19 impacts on individuals and their households. In the positive change domain (Fig1d), participants reported the following individual impacts most frequently: being more appreciative of things usually taken for granted (84%) and paid more attention to personal health (84%).
Table 2: COVID-19 impacts at individual and/or household levels by participant health literacy level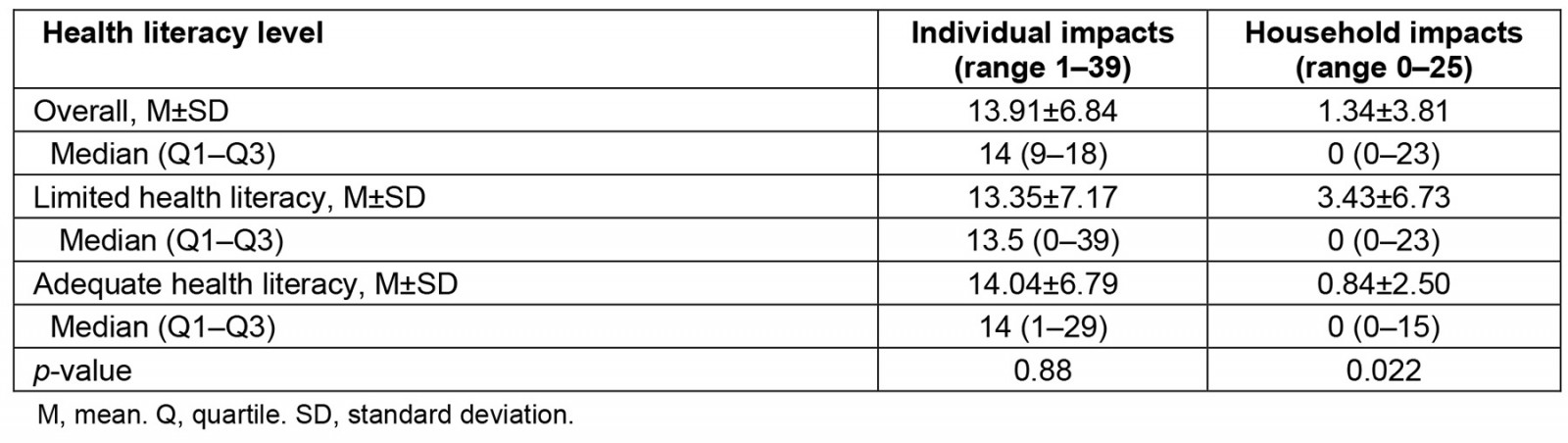
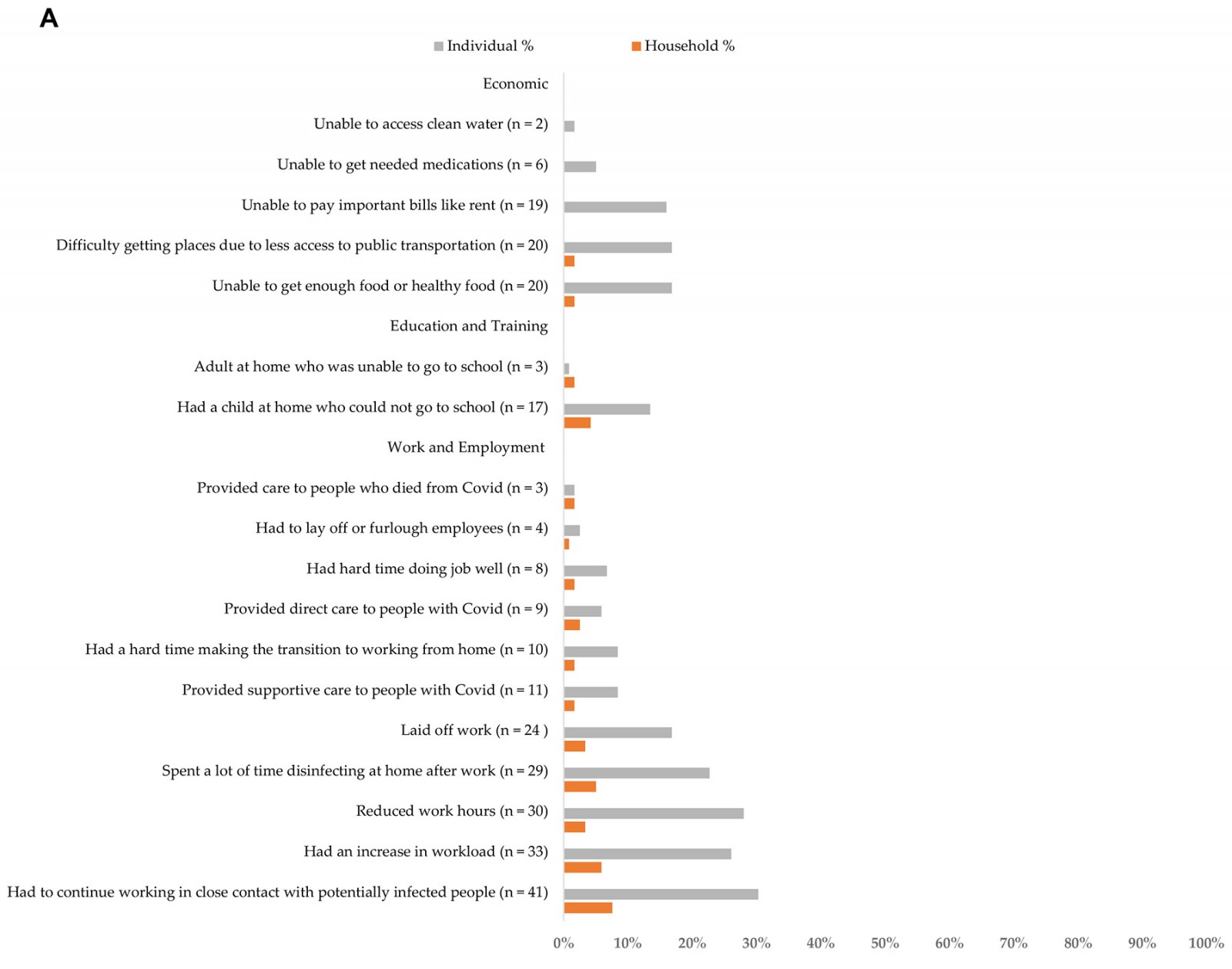
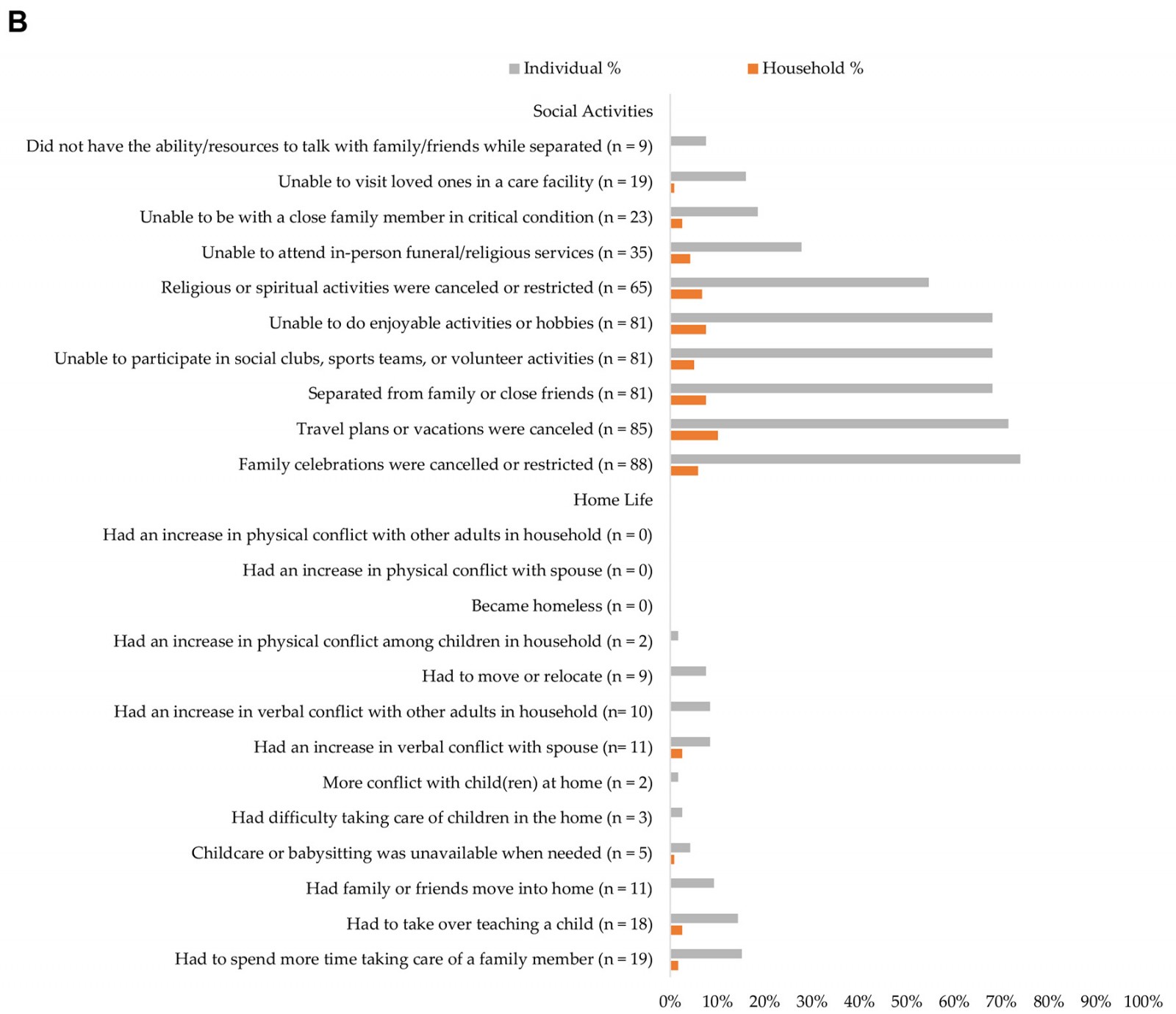
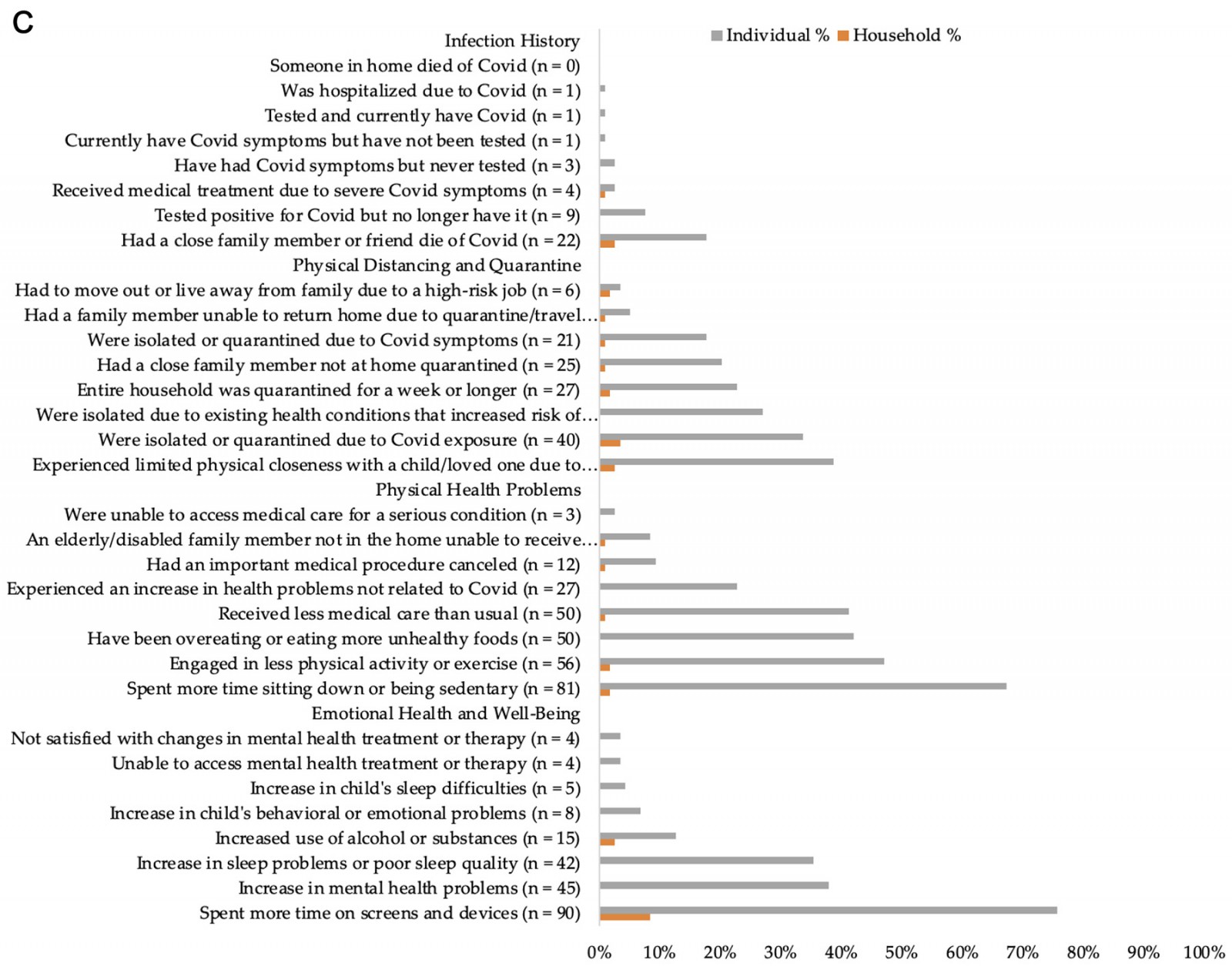
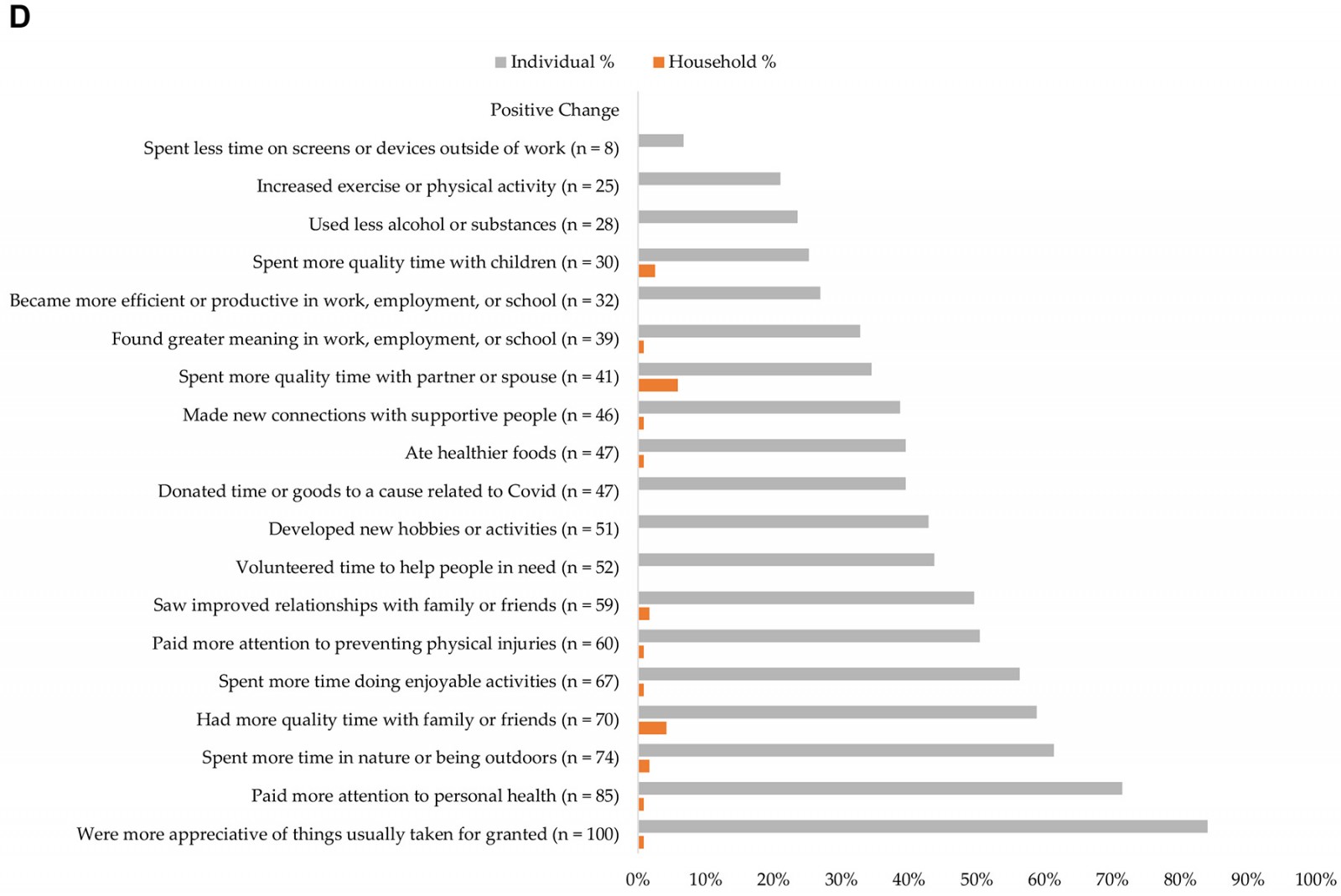 Figure 1: Frequency of COVID-19 impacts in the domains of (A) economic, education and training, and work and employment; (B) social activities and home life; (C) infection history, physical distancing and quarantine, physical health problems, and emotional health and wellbeing; (D) positive change.
Figure 1: Frequency of COVID-19 impacts in the domains of (A) economic, education and training, and work and employment; (B) social activities and home life; (C) infection history, physical distancing and quarantine, physical health problems, and emotional health and wellbeing; (D) positive change.
Bivariate results on health literacy and COVID-19 impacts
As shown in Table 2, health literacy level was not significantly associated with individual COVID-19 impacts. Participants with limited versus adequate health literacy did, however, report more household impacts on average (3.43 versus 0.84, p=0.022). Results for each COVID-19 pandemic impact domain showed that participants with adequate versus limited health literacy reported significantly more individual social impacts on average (4.97 v 3.78, p=0.034). The opposite was found for household social impacts: participants with limited versus adequate health literacy reported more household social impacts on average (1.26 v 0.32, p=0.024). Participants with limited versus adequate health literacy also reported more household emotional health and wellbeing impacts (0.30 v 0.07, p=0.026), as well as more household infection history impacts (0.13 v 0.01, p=0.045) on average.
Multivariable results on health literacy and COVID-19 impacts
As shown in Table 3, health literacy level was not significantly associated with the rate of individual COVID-19 impacts controlling for covariates (incidence rate ratio (IRR) 0.84, 95%CI 0.67–1.06, p=0.14). The biological sex of participants (male v female) and health insurance type (having public insurance versus any private insurance) were each associated with a lower rate of individual-level COVID-19 impacts. Conversely, participants who did not identify as White and non-Hispanic had a significantly higher rate of individual COVID-19 impacts. In terms of household COVID-19 impacts, health literacy level was the only factor with a statistically significant association. That is, participants with limited versus adequate health literacy had a higher rate of household COVID-19 impacts (IRR 5.89, 95%CI 1.82–19.1, p=0.003), after adjusting for covariates.
Results from the sensitivity analysis of the three household COVID-19 impact domains (social, emotional, infection) showed, that for each domain, limited health literacy was associated with a higher adjusted rate of household impact in each domain (social COVID-19 impact domain IRR 7.21, 95%CI 2.11–24.66, p=0.002; emotional COVID-19 impact domain IRR 5.17, 95%CI 1.42–18.77, p=0.013; infection COVID-19 impact domain IRR 14.78, 95%CI 1.79–121.79, p=0.012). Model results for the household social COVID-19 impacts additionally revealed a statistically significant association with being male versus female (IRR 3.34, 95%CI 1.21–9.24). Having public insurance or being uninsured was associated with a lower rate of household infection impact (IRR 0.17, 95%CI 0.03–0.90, p=0.037).
Table 3: Multiple negative binomial regression model results for COVID impacts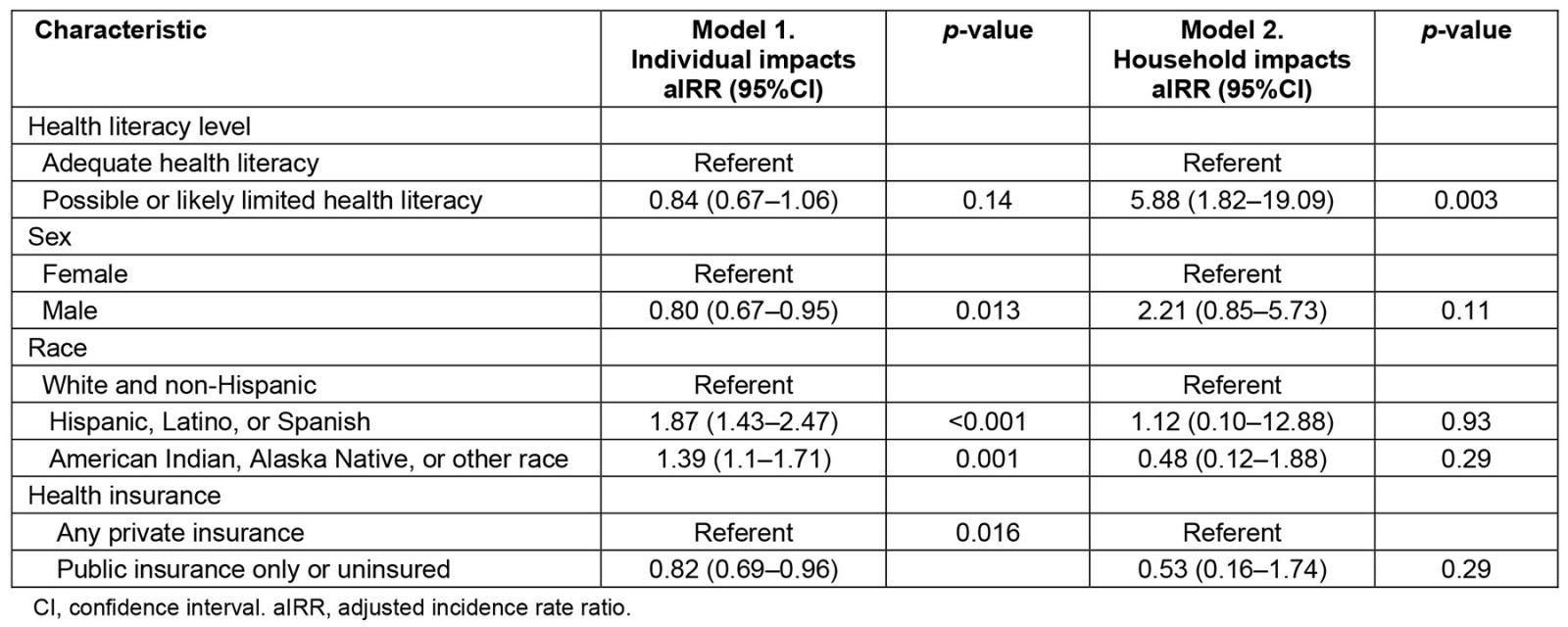
Discussion
This study is one of the first to examine associations of health literacy with COVID-19 pandemic impacts on various aspects of personal and family life in a diverse sample of adults living in a rural region of the Southwestern US. Adults in this study’s sample were found to have had approximately 22 individual impacts and 2 household impacts of the total 92 COVID-19 pandemic impacts that were assessed. COVID-19 pandemic impacts relating to positive change, emotional health and wellbeing, social activities, and physical health problems were commonplace. Although both bivariate and multivariable analysis showed that participant health literacy level was not significantly associated with individual COVID-19 pandemic impacts, health literacy level was significantly associated with household COVID-19 pandemic impacts. Specifically, limited versus adequate health literacy was associated with more household COVID-19 pandemic impacts on average. Sensitivity analysis results additionally suggest that limited health literacy may be most strongly associated with household social, emotional, and infection impacts. Because household COVID-19 pandemic impacts were reported less frequently than individual impacts overall, household impacts may be indicative of a greater burden or hardship brought about through the pandemic.
Our study’s findings showed that a higher percentage of participants who identified as being BIPOC had limited health literacy and that being BIPOC versus white and non-Hispanic was associated with having more individual COVID-19 pandemic impacts on average, which is similar to a recently published research on associations of race and ethnicity with health literacy and COVID-19 vaccine confidence12. Although several recent studies show that adequate health literacy is protective in terms of COVID-19-related beliefs14,27, knowledge13, and behaviors16,17,28, this study’s findings did not show adequate health literacy was significantly associated with individual COVID-19 pandemic impacts. Our study’s results also suggest that identifying as male versus female and having public versus private health insurance is related to fewer individual COVID-19 pandemic impacts. This study’s results relating to men possibly faring better in terms of individual-level COVID-19 pandemic impacts may be explained, in part, by prior research showing females were more likely than males to have mental distress and greater social, financial, and medical impacts during the pandemic29. It is additionally possible that some information bias may have been at play as far as men may have felt more societal pressure to report fewer individual impacts than women during a crisis such as the COVID-19 pandemic. Furthermore, being male versus female was associated with a higher rate of household social COVID-19 impact, suggesting that males may have experienced greater impacts in certain domains and plausibly felt more comfortable reporting this type of impact at a household versus an individual level. Future research is also needed to tease apart how other household and individual characteristics such as the number of household members and marital status may contribute to the gender effects found in this study (eg marital status and number of household members may modify associations of health literacy with individual and/or household impacts). The health insurance findings may be partly due to more than one-third of our study’s sample being aged 65 years or older and therefore eligible for Medicare, as their public insurance; that is, public insurance in this study was not necessarily a marker of poverty but rather age.
This study’s findings suggest that the use of health literacy screening with the Newest Vital Sign or other time-efficient tools in clinical settings could help to identify individuals who are at the highest risk for adverse impacts brought about through epidemics, pandemics, and other emergency events such as natural disasters (eg hurricanes, wildfires). Greater risk mitigation potentially involving emergency preparedness education and other related measures may be undertaken to help individuals with limited health literacy better optimize their health in the face of adversity. Maintaining a universal precautions approach in tailoring and delivering such health education and promotion initiatives (ie approaching everyone as though they may have limited health literacy) will remain essential30. Adopting innovative approaches to deliver health education such as mobile health (mHealth) options, including gaming through phone apps, may also be a promising approach to building electronic health (eHealth) literacy and reducing risk related to limited health literacy in crises31. Intervention models to enhance health literacy and health consciousness in crises may also help to reduce adverse impacts and address infodemics. Some recent research additionally indicates that interventions incorporating peer-to-peer learning and other trusted sources to deliver health education may be especially helpful in increasing health literacy related to the COVID-19 pandemic32,33.
It is also important to address the current shortage of healthcare professionals across the country, especially in Northern Arizona. Healthcare professionals (eg primary care, dental health, and mental health) play an important role in counseling individuals regarding their health as well as the impact of pervasive health-related problems such as COVID-1934. Areas where these shortages are most concentrated are Health Professional Shortage Areas (HPSAs). The Health Resources and Service Administration reports that there are around 74 million people living in 7456 HPSAs nationwide with 613 of those areas belonging to Arizona alone35. Health literacy-boosting interventions targeting clinicians and trainees may also be important during epidemics and pandemics to reduce the spread of misinformation36 and to help ensure healthcare workers take recommended infection control precautions themselves37.
Limitations
Despite drawing random samples of adult patients from two federally qualified health centers in Northern Arizona, this study’s sample self-selected (opted in) to participate. This may, in part, explain the older age and the lower percentage of adults (19.3%) in our sample with limited health literacy than found in the general US population10,38,39. Nevertheless, our sample had considerable racial and socioeconomic diversity with approximately 23% of participants identifying as American Indian or Alaska Native, and 52% having public health insurance. Of note, 37% of participants were 65 years or older, which may be important to consider regarding their likely enrollment in Medicare (public insurance regardless of income level). Another limitation of our study is that we did not measure all factors potentially contributing to health literacy and individual and household COVID-19 pandemic impacts (eg household income, participant education, political ideology). We also did not measure COVID-19 or epidemic/pandemic health literacy more specifically, which may have contributed to the nonsignificant association between the general health literacy level measured by the Newest Vital Sign and individual COVID-19 pandemic impacts. Adapting health literacy measures relevant to epidemic/pandemic contexts is an area in which future work is needed40. Along these lines, we did not examine certain COVID-19 pandemic-related outcomes such as COVID-19 beliefs, knowledge, and behaviors such as vaccine hesitancy or refusal. This may also be a strength of our study as far as we examined many other pandemic impacts.
Conclusion
This study was one of the first to examine associations of health literacy with individual and household COVID-19 pandemic impacts among adults in a rural area of the United States. Biological sex, race and ethnicity, and health insurance type were each significantly associated with individual COVID-19 pandemic impacts. Limited health literacy was significantly associated with higher household COVID-19 pandemic impacts on average. Findings reinforce that health literacy is important to address in preparing for and mitigating impacts from emergency events.
Acknowledgements
We acknowledge the assistance of Ivonne Garber and Levi Stidham with recruitment and data collection for this study.
Funding
We also acknowledge the funding support for this project that was provided by the Southwest Health Equity Research Collaborative at Northern Arizona University (U54MD012388), which is sponsored by the National Institute on Minority Health and Health Disparities (NIMHD).
Conflicts of interest
The authors have no conflicts of interest to declare.