

Introduction
The Democratic Republic of Timor-Leste is situated on the island of Timor, approximately 700 km north-west of Darwin, Australia. Most (71%) of Timor-Leste’s 1.2 million population live in rural areas, with around half living in the more remote areas isolated by mountains and poor roads1. The capital of Timor-Leste is Dili and the official languages are Tetum and Portuguese, with English and Indonesian as working languages. Away from Dili there is almost total reliance on subsistence agriculture, with small landholders having little or no access to markets. Timor-Leste is divided into 13 municipalities, of which one is a special administrative region; there are 65 subdistricts and 442 sucos (villages). Decentralisation is under way to give greater control at the district (local government) level; this includes responsibility for primary health care. Aileu, a rural municipality, is spread across approximately 700 km2 of mountainous area to the south of the capital, Dili and has a population of 48 500 people (2015)1. Aileu municipality comprises the remote subdistricts of Laulara, Liquidoe and Remexio2. Most families in Aileu rely heavily on subsistence farming, and access to water, sanitation, electricity, health services, education and employment is limited across the municipality.
Since independence in 2002, Timor-Leste has made progress in building a peaceful democratic nation, living standards have improved, and healthcare services, food security, improved sanitation, and agriculture and education facilities have been established. However, the 450 years of foreign occupation, complicated by periods of political instability and internal violence, continue to challenge the rebuilding process and efforts. Much of the recent investment has been used to rebuild the infrastructure destroyed during the lead-up to independence. During 1999, 35% of all health facilities, including almost all dental infrastructure, and 80% of schools were destroyed. This level of destruction applied to roads, water, electricity and communications infrastructure3.
Although poverty is decreasing, unemployment is high (40%) and Timor-Leste remains one of the poorest countries in the region, with 41.8% of the population living below the poverty line4. A priority as the country rebuilds is to protect public health, and achievements have been made in reducing infant, child and maternal mortality, improving nutrition and controlling infectious disease through immunisation, clean water and malaria programs5. Oral health, although not a key health priority, impacts on general health and can result in morbidity, economic burden and reduced quality of life6. Dental caries is a progressive disease which if not managed results in pain, the loss of tooth structure and ultimately function and quality of life7. In addition, poor oral health and toothache are linked with school absence and decreased academic performance8.
Despite a major reconstruction program and improvements in access to health services, the oral health situation in Timor-Leste is alarming, with high caries prevalence rates of 72% reported for children aged 6 years; children aged 12 years had on average a decayed, missing and filled (DMFT/dmft) score of about 2, with 66% being untreated decay9. More recent evidence indicates that the oral health for children in the capital of Dili is deteriorating, with 40% of school children experiencing toothache during 201410. Dental caries is a preventable disease, with diet, access to fluoride and toothbrushing being well-documented factors associated with preventing caries development7. In Timor-Leste, dietary behaviour is affected by both demand and supply influences. Import data confirms that Timorese have easy access to sugar: there was a 149% increase in the volume of sugar coming into the country between 2003 and 201411. Changes in traditional diet due to this ease of availability of sugar may be more pronounced in Dili; however, anecdotal data on oral health suggest a similar effect in the rural/remote subdistrict areas12. Irrespective of easy access to sugar, food security is still a problem in Timor-Leste, with 34.3% of people experiencing undernutrition13. The indicators for chronic malnutrition are also still high, with 46% of all children under 5 years stunted and 24% with signs of wasting (thin for height)14. There is no water fluoridation in Timor-Leste and because all toothpastes sold contain fluoride, teeth brushing becomes the de facto measure of fluoride exposure. In a recent survey of urban Timorese children, 75% self-reported brushing regularly with toothpaste12. However, access to fluoride toothpaste in rural/remote areas of Timor-Leste is undocumented.
There is a lack of epidemiological data on dental caries estimates for the rural/remote areas of Timor-Leste and such data are required to inform oral health issues and health policy at both local and national levels.
This study investigated the caries status and potential risk factors among primary school children in the rural Aileu municipality and its remote submunicipalities in Timor-Leste. The study objectives were to:
- determine caries prevalence and experience
- determine the status of existing caries lesions – active or arrested
- identify associations between dental caries and potential risk factors.
Methods
This study analysed secondary data. The de-identified data for this analysis were obtained from North Richmond Community Health (NRCH), Melbourne, Australia.
NRCH has been working with the Friends of Aileu (a government-to-government partnership between an Australian local government area and the municipality of Aileu) to improve the oral health of school children in the municipality of Aileu. NRCH conducts an outreach school-based oral health promotion program, called Kose Nehan, at six primary schools in the Aileu municipality. This program includes dental check-ups for all children at participating schools; oral health education for school staff, delivered twice a year by a local dental nurse; and supervised (by teachers) daily teeth brushing at the school for the children, using standard fluoride toothpaste.
Participating primary schools were selected by the municipality administration (convenience sample) to represent the three remote subdistricts of Aileu municipality: Laulara, Remexio and Liquidoe. The selection was primarily based on remoteness and access to dental services located in Aileu, the main township in the rural Aileu municipality (ie the most remote schools were selected). All children at selected schools were invited to participate. NRCH conducts its outreach program in Timor-Leste with the understanding and written informed consent of each child, the school teachers and the school principal, after thoroughly and clearly explaining all aspects of the study to the children (under supervision of school staff) and according to the World Medical Association Declaration of Helsinki.
For this study, using an absolute precision-based sample size calculation, it was estimated that 369 children were required to detect an absolute precision of 0.05 (±5%; 95% confidence interval (CI) of 35–45%) around a parameter estimate of 0.40 (caries prevalence of 40%). The parameter estimate was obtained from a recent study10.
Caries was diagnosed using the International Caries Detection and Assessment System (ICDAS)15. ICDAS enables measurement of the progressive caries process compared with other systems, which only record dentinal lesions (cavities). Children were examined in the school setting, lying down on a bench with their head on the examiner’s lap. Air-drying of teeth using compressed air was not used as this was considered impractical in the field setting. The omission of this ICDAS step enabled the use of ICDAS caries code 1 only in the pit and fissures (and not on the smooth surface). Caries lesion activity status (active/inactive) was recorded and defined using criteria proposed in the International Caries Classification and Management System guideline16. Examiners were trained and calibrated. Following a training session using photographs of caries lesions in the ICDAS e-learning training program17, dental examiners and the reference standard jointly discussed presentation of caries lesions and the corresponding codes, until consensus was reached. This was followed by a calibration exercise. The kappa score for inter-examiner reliability was 0.70 (95%CI of 0.54–0.85) and for intra-reliability was 0.90–0.92. A brief interviewer-administered (school or Kose Nehan staff) questionnaire was used to capture information on child oral hygiene and diet behaviours.
For this analysis, 2016 data on dental caries and associated factors for 685 primary school children from the six participating primary schools were obtained. Caries estimates were reported as the dmft (primary dentition) or DMFT (permanent dentition) score and reported separately for the primary and permanent dentitions. Three definitions of the ‘d’ component of the dmft/DMFT index were used: (i) any caries lesions (ICDAS caries scores 1–6), (ii) the WHO cavitated ‘d’ lesions (ICDAS 3–6)18 and (iii) extensive cavities only (ICDAS 5–6). For the descriptive analysis, estimates were reported as the caries prevalence (proportion of children with disease) and caries experience (average number of lesions per child) of dental caries. Caries experience was reported as the mean (SD) and median scores (interquartile range (IQR)). The median measure of central tendency was included because the mean for caries data is often positively skewed and as such does not reflect the true central estimate. Correlation between potential explanatory variables were explored to eliminate redundant information. Multivariable logistic regression analysis, modelling the odds of having caries (any caries lesions – ICDAS caries codes 1–6), was then conducted to identify independent predictors of caries in this sample. For this analysis, the dichotomous outcome was caries experience (dmft/DMFT) yes/no. This analysis was conducted separately for the primary and permanent dentitions. The multivariable analysis was first used to compute partially adjusted odds ratios (OR) and 95%CI, adjusted for child age and sex. This was done to study the individual effect of each potential predictor on the outcome and to guide decisions on variables to include in the final model. This final adjusted analysis accounted for the simultaneous effect of potential predictors to study their independent effect on the outcome. The clustering effect of the outcome, by school, was accounted for in the analysis. Data were analysed using Stata v14 (StataCorp; http://www.stata.com).
Ethics approval
An ethics exemption for secondary data analysis was obtained from Deakin University’s Human Research Ethics Committee.
Results
This sample of 685 primary school children consisted of equal numbers of female and male children. There were no gender differences between male and female children for caries prevalence in the deciduous and permanent dentition across all caries severity levels (Tables 1,2).
Primary dentition
In the primary dentition of children the overall prevalence of caries (any caries lesions) was 64%, the mean dmft score (any caries lesions) was 2.74 (SD 3.08) and the median dmft score was 2 (IQR 0–5) (Table 1); for the WHO index age of 6 years, caries prevalence was 75% and the mean dmft score was 4.17 (SD 3.75) and the median dmft score was 4 (IQR 0–7) (Table 1). Variations in caries prevalence and experience scores were observed across the six schools.
Table 1 shows that the overall caries prevalence (any caries) in the primary dentition (ICDAS 1–6) was 64%, decreasing to 61% for any cavitated lesions (ICDAS 3–6); and 52% for extensive lesions involving dentine (ICDAS 5–6). This implies that almost 80% (79.7%) of the cavities in the deciduous dentition were extensive lesions. In the permanent dentition, this translates to 43.4% of cavities in the permanent dentition being extensive lesions. The caries prevalence in the deciduous dentition increases with age between 6 years and 8 years and decreases slightly from ages 9 years to 11 years. Figure 1 shows that the majority of carious lesions were active.
Table 1: Caries estimates for primary dentition by demographics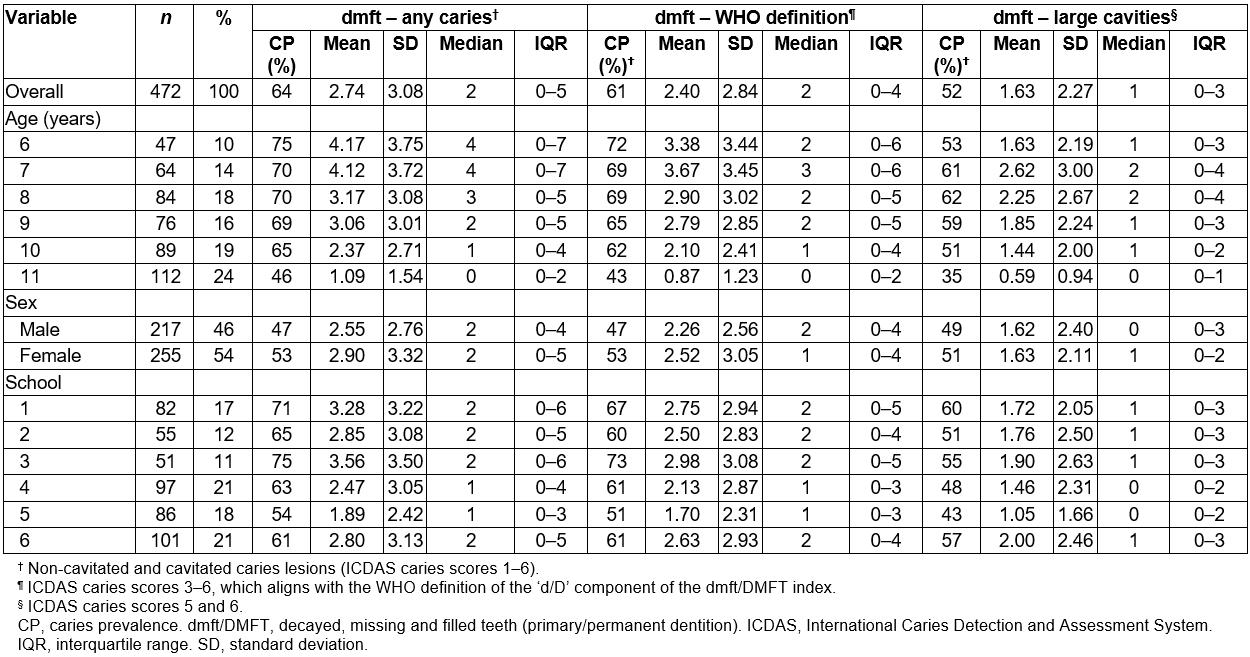
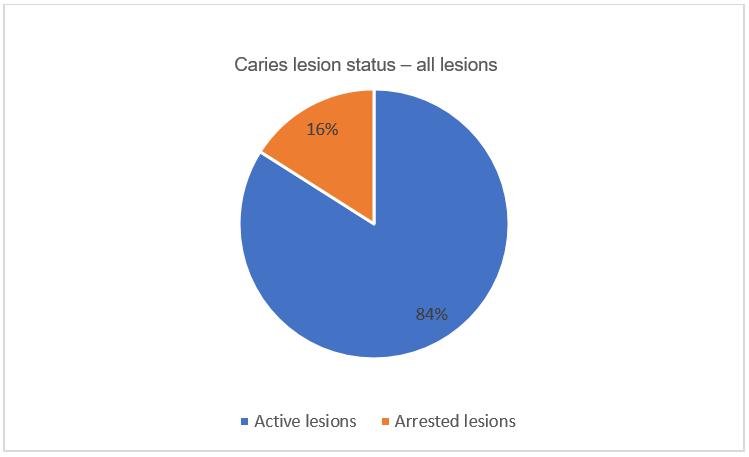 Figure 1: Caries lesion activity status for all caries lesions (ICDAS 1–6) in primary teeth of children aged 6–11 years.
Figure 1: Caries lesion activity status for all caries lesions (ICDAS 1–6) in primary teeth of children aged 6–11 years.
Permanent dentition
In the permanent dentition of children, the overall prevalence of caries (any caries lesions) was 53%, the mean DMFT score was 1.74 (SD 2.46) and the median DMFT score was 1 (IQR 0–2) (Table 2); for the WHO index age of 12 years, caries prevalence was 51% and the mean DMFT score was 1.32 (SD 1.75) (Table 2). When caries was defined as cavities or large cavities, the mean DMFT scores for children aged 12 years were 0.64 (SD 1.26) and 0.42 (SD 0.91), respectively (Table 2).
‘Any caries’ prevalence was highest at age 14 years, increasing from 50% to 56%. (Table 2)
Table 2: Caries estimates for the permanent dentition by demographics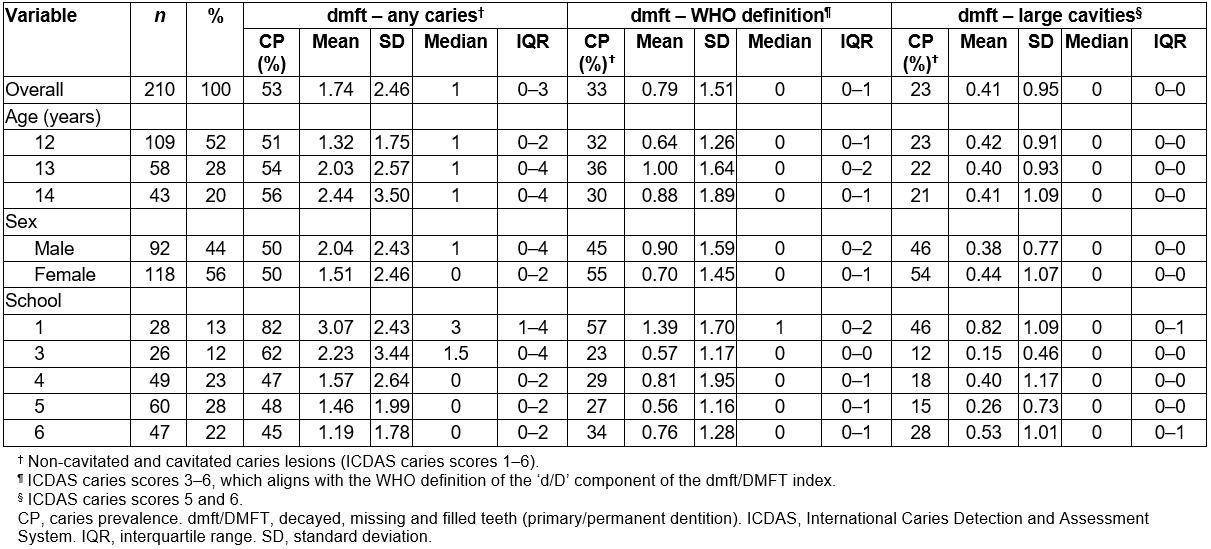
Comparison of caries prevalence in primary and permanent dentition by primary school
A perceived difference in caries prevalence in the deciduous dentition was noted between the primary schools included in this study, ranging from caries prevalence of 45% in school 6 to 82% in school 1 (Table 2). Similarly, it was noted that there is a perceived difference in caries prevalence in the permanent dentition between the primary schools included in this study ranging from caries prevalence of 45% for school 6 to 82% for school 1 (Table 2). Substantial variations in mean dmft/DMFT scores were observed across schools for both the primary and permanent dentitions.
Caries lesion activity status
Studying caries lesion activity status, for all three reported definitions of caries, approximately 84% of lesions were identified as being active carious lesions. This was also observed across both the primary and permanent dentitions (Fig1).
Association between exposure to risk factors and caries prevalence
In the multivariable regression analysis, none of the included exposure variables had an independent significant effect on the outcome (Table 3).
Table 3: Logistic regression analysis to identify independent associations between exposures and dental caries in primary and permanent dentitions of children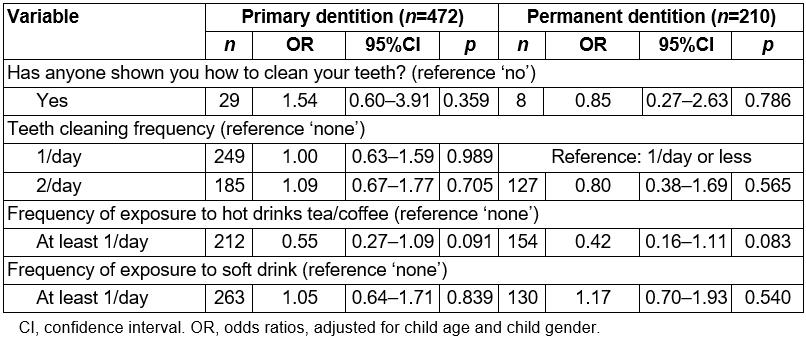
Discussion
This study reports on caries prevalence and caries experience of Timorese children attending six rural/remote primary schools. The study also reports on the potential risk factors for dental caries in this population group.
The results of this study support the findings from current published literature, which indicates that dental caries status among Timorese primary school children is high and on the increase in the permanent dentition10. The results of this study also indicate that most of these lesions are active and cavitated.
Differences in the prevalence of dental caries were perceived between primary schools, ranging from 54% to 71% for the primary dentition and 45% to 82% for the permanent dentition. Further investigation into the factors that may influence these noted caries prevalence differences between and within schools is required.
The data in tables 1 and 2 indicate that strategies for the prevention of dental caries in children in Timor-Leste need to be implemented at different stages of child development: antenatal, in the early years of child development and during the school-age years. In this way, oral health behaviour changes are encouraged by the primary carer in the early years of a child’s life and reinforced as the child grows and develops. Such programs should include well baby dental check-ups, anticipatory oral health guidance with regard to appropriate use of bottle feeding (supervised and not prolonged use during sleep), promotion of consumption of cariogenic foods and drinks during meal times and not as in-between meal snacks, twice-daily teeth brushing using a smear of standard fluoride toothpaste and applications of fluoride varnish twice a year by dental and non-dental health professionals.
By age 6 years the caries prevalence is high, with extensive carious lesions accounting for 80% of all cavitated lesions. Primary-school-based oral health promotion strategies are unlikely to be effective in reducing the prevalence and severity of dental caries in the primary dentition of children aged 6 years; but are more likely to reduce the caries prevalence in the permanent dentition in children older than 6 years. Based on the recommendations of the 2016 WHO report Promoting oral health in Africa19, Timor-Leste needs to promote oral health at the community level with the following messages.
1. Oral diseases and conditions are highly common in Timor-Leste
Local data should be provided to the community to demonstrate that children in this community are highly affected by the dental caries condition. Discussion of local risk factors that contribute to the high prevalence of dental caries among young children should be widely understood by the community, including the impact of malnutrition on oral health and vice-versa. The World Food Programme 2018 indicated that, irrespective of the accessibility of sugar, food security is still a problem in Timor-Leste, with 34.3% of people experiencing undernutrition13. The UNFPA annual report for 201614 reported that the indicators for chronic malnutrition are also still high, with 46% of all children aged less than 5 years being stunted and 24% with signs of wasting (thin for height). Sheetal et al state that ‘Malnutrition affects the oral health and a poor oral health in turn, may lead to malnutrition’20. Other studies have suggested that malnutrition can lead to enamel hypoplasia/hypomineralisation, salivary gland dysfunction and saliva compositional changes21, all of which are associated with increased risk for dental caries. Because chronic malnutrition is high amongst children in this population group, this factor may mask the impact of caries-specific risk factors such as increased frequent consumption of sugar products. Furthermore, the large prevalence of extensive caries lesions in both the primary and permanent dentition can exacerbate malnutrition due to difficulty in eating associated with toothache from extensive carious lesions.
2. Dental caries can be prevented from childhood
Communications about prevention of dental caries should be implemented by dental and non-dental health professionals during the antenatal and postnatal periods and should include the promotion of affordable fluoride toothpaste to prevent dental decay for the child and family, oral health activities in local schools, and engagement with local intersectorial partnerships/collaborations. Culturally relevant and affordable oral health interventions, targeting children (at different stages of their development) and their carers, need to be developed in collaboration (through co-design processes) with key stakeholder groups and consumers. The implementation of culturally relevant oral health interventions may prove difficult. However, if key Timor-Leste stakeholders and consumers are involved in all stages of design, implementation and evaluation of these interventions, identified barriers to the success of these interventions may be overcome.
3. Prevention of oral diseases begins at home
Oral health education for individuals and families about oral hygiene and teeth brushing with fluoride toothpaste should be circulated widely, with special efforts to reach remote, uneducated and otherwise vulnerable audiences18. This information should be included with other basic health promotion messages emphasising health-promoting behaviours, including healthy diets.
4. Much treatment can – and should – be done locally
Community members should be encouraged to attend their local health centre or seek help from qualified oral health professionals when symptoms appear. For those children with existing non-extensive dental decay, atraumatic restorative treatment can be used to treat the existing lesions with glass ionomer cement restorative materials and prevent further decay by sealing pits and fissures at risk of dental caries with the same restorative material. Furthermore, consideration should be given to the use of the Hall crown technique for deciduous molars affected by non-extensive dental decay (ie carious lesions that are unlikely to extend beyond the middle third of dentine)22. The Hall crown technique has been shown to be highly successful in comparison to conventional restorations23. For those children with advanced dental caries, there is a need to ensure that emergency dental services aimed at pain relief, first aid for oral infections and trauma to the mouth and face, and referral of complicated cases to the nearest hospital or oral health professional, are available.
Study limitations
The results of the multivariable regression analysis demonstrated lack of an independent significant effect on dental caries related to exposure to known cariogenic factors, although trends in expected directions were observed. The high prevalence of chronic malnutrition amongst children in this population group13 (although not recorded in the NRCH program) is likely to be a confounding factor that may be associated with caries and may be masking the impact of known cariogenic risk factors on caries development.
The cross-sectional nature of the study limits the interpretation of the results to the timeframe when the data was collected. Furthermore, the schools in the study demonstrated significant differences in the prevalence of dental caries for the primary dentition and for the permanent dentition. The sociodemographic characteristics of the children attending each of the schools included in the study were not collected. Future studies should include collection of sociodemographic characteristics of the schools including the factors that may have influenced these noted caries prevalence differences between and within schools. The overall sample size of primary school children included in the study met the sample size calculations requirements reported in the methodology section. However, when the overall sample size was subdivided into age groups, the number of children in each of the age groups was small.
The confounding factor of chronic malnutrition was not factored in the design of the study. This may have impacted on the findings of this study and masked the impact of known cariogenic risk factors on caries development. Furthermore, the high prevalence of extensive caries lesions in both the primary and permanent dentition may exacerbate chronic malnutrition due to difficulty in eating associated with toothache from extensive carious lesions, and needs further investigation. It should be noted that the use of ICDAS without air drying with compressed air eliminated the ICDAS caries code 1 on the smooth surfaces and those in the pits and fissures that would have only been visible after drying. As such, the caries estimates reported in this study may have been underestimated. Despite this limitation, the caries information reported in this study is a more accurate estimation of the true population value, compared with other studies that report on dental caries at the level of cavitation.
Conclusions
The key finding is that the caries prevalence (any caries) of the children in the study group, in both the primary (ages 6–7 years) and permanent dentition (ages 12–13 years) is high.
Malnutrition, which was not measured for this study, is highly prevalent among children in Timor-Leste and could explain the high caries rates in this population. The effect of malnutrition on dental caries and vice-versa needs further investigation. Programs and policies are urgently needed for oral health promotion and also the prevention and management of dental caries in Timorese children. These strategies should also address the urgent need for emergency dental services aimed at pain relief, first aid for oral infections and restorations, given the high prevalence of advanced disease in this child population.
Acknowledgements
NRCH acknowledges the funding support from the Borrow Foundation to evaluate the Kose Nehan program.