


Introduction
The recruitment and retention of healthcare professionals to live and work in rural and remote areas is a global challenge1. Effective recruitment and retention of healthcare professionals is required to ensure a stable workforce, strong patient–healthcare professional relationships, continuity of care and optimal health outcomes2. Rural and remote communities often experience a high turnover of healthcare workers3. This can exacerbate problems associated with access to healthcare services and increase the direct and indirect costs of health care3.
Pharmacists are a group of allied health professionals that play a vital role in both the clinical and community setting4. Aside from dispensing, pharmacists contribute their expertise on matters related to medication selection, rational use of medication and medication safety4. Those in community settings are also involved in the triage and referral of clients to clinicians and other allied health professionals5. Pharmacists, especially those practising in community settings, are an easily accessible group of healthcare professionals and often the first point of contact into the healthcare system for many patients4,5.
In less than 20 years, the number of pharmacists in Australia more than doubled from around 13 000 to 31 955 in 20196. This has been associated with an increase in the number of pharmacy schools delivering entry level pharmacy programs from six in 2002 to 18 as at 20207. Two drivers are in part responsible for this increase: a global shortage of pharmacists since the early 1990s8; and the report by the Australian Institute of Health and Welfare in 2003 suggesting a local shortage of pharmacists that is expected to continue beyond 20109,10. Despite reports suggesting an oversupply of pharmacists11,12, there is currently an inadequate supply in rural and remote areas13. Despite the presence of approximately 5700 widely distributed community pharmacies, those outside of metropolitan areas find it consistently difficult to attract, recruit and retain pharmacists14. This can lead to a reduction in pharmacy services for an already vulnerable population. Limited research within the Australian context has, however, focused on the strategies for increasing rural and remote pharmacist workforce. This is important, given that pharmacists in rural and remote areas serve a different and often disadvantaged communities where the population15may be socioeconomically disadvantaged and have limited health literacy16. Therefore, an extensive scoping review of the current literature related to this theme is required to identify strategies for increasing the pharmacist workforce and factors associated with retention in rural and remote Australia. Over the years, several geographical classification systems have been utilised. These include the Accessibility/Remoteness Index of Australia (ARIA), ARIA+, Australian Standard Geographical Classification-Remoteness Area (ASGC-RA) and the more recent Modified Monash Model (MMM) classification17. Due to nuances in the various classification systems utilised over the years, and for the purpose of this article, ‘rural and remote’ was defined as non-metropolitan locations.
Methods
Study design
Scoping reviews are used to provide a broad overview and investigate under-studied topics, although they may subscribe to slightly different methods and procedures18,19. This review adopted a staged framework with the following steps: (i) identifying the research question, (ii) identifying relevant studies, (iii) study selection and (iv) charting the data20.
Search strategy
An electronic search of Ovid Medline (Medline and Embase), CINAHL and Scopus records was conducted to investigate strategies for increasing the rural and remote pharmacist workforce and factors associated with the retention of pharmacists in rural and remote Australia. The search terms included a combination of Austra* AND (rural OR remote) AND (health*) AND (recruit* OR retain* OR retention*) AND (Pharm*).
Eligibility criteria
Articles eligible for consideration included review articles, cross-sectional studies, or any other study design, published in the English language and in a peer-reviewed journal, indexed in Ovid Medline (Medline and Embase), CINAHL or Scopus. For inclusion, articles had to be focused on pharmacists alone or in combination with other healthcare professionals and published between January 2000 and August 2019. Articles were required to be focused on a defined strategy designed to increase the rural and remote pharmacist workforce, or factors associated with the retention of pharmacists in rural or remote areas. Excluded were editorials, letters, commentaries, books and book chapters. Studies conducted outside of Australia were excluded.
Study selection
On completion of the databases search, all citations were exported into the EndNote X7 (Thomson Reuters; https://support.clarivate.com/Endnote/s/article/EndNote-Installer-download?language=en_US) reference management software and duplicates were removed. In the first stage, two authors independently screened the titles and abstracts for eligible articles using the inclusion and exclusion criteria. Articles were retained where both reviewers agreed met the eligibility criteria. For the second stage, both reviewers again independently screened the abstracts of disputed articles. Where consensus could not be reached, a third reviewer independently screened the residual articles for inclusion or exclusion. Articles identified from the reference list and texts of included articles were also considered for inclusion. Articles not retrieved from the search but recommended by the research team or reviewers were also to be included if they met the inclusion criteria.
Data extraction process
Data extraction was performed by one of the investigators using a prepared table with the headings Author, Location, Study design/number of participants, Personal factors/perception Workplace and Community. The extraction sheet was designed to enable comparison as well as a synthesis of information across articles. Strategies for increasing rural and remote pharmacist workforce were operationalised as current or proposed approaches to engage the services of pharmacists in rural or remote areas, or reasons why pharmacists have decided to practise in a rural or remote location. Factors affecting retention were defined as positive or negative reasons why pharmacists choose to remain or leave rural or remote locations. Factors associated with retention were mapped to personal, workplace-related or community factors. No formal quality assessment of the included studies was conducted. This approach is consistent with established guidelines for scoping reviews18,20.
Results
The literature search yielded 105 articles (Fig1). After removal of duplicates, 56 articles remained. At the first stage, seven articles were retrieved; there were two articles in the second stage and no articles were referred to a third reviewer. Three articles were retrieved from the reference list of identified articles, while one additional article was suggested for inclusion by an external reviewer. Strategies were either related to the preparation of students for rural pharmacy practice or the recruitment of rural pharmacists. Those related to the preparation for rural practice included establishment of pharmacy schools in rural areas21-23, inclusion of rural content in university teaching curriculum23-25, availability of support personnel for rural initiatives24, enrolment of students from rural backgrounds26-28 and rural placements25,26,29,30.
In Australia, students aspiring to become pharmacists need to complete a degree program that is accredited by the Australian Pharmacy Council, followed by a 1-year supervised practice in an approved setting7. The focus on pharmacy education and training in non-metropolitan areas is expected to increase the pharmacy workforce in such areas23.
Only one study focused on the actual recruitment of pharmacists to a rural location31. This may be related to the difficulty in recruiting and retaining pharmacists in non-metropolitan locations5. In Australia, 63% of pharmacists work in community pharmacies, while 18% work in a hospital setting32. Of these numbers, only an estimated 23% work outside a metropolitan setting33.
A number of factors associated with retention were also identified and mapped to personal, workplace or community factors (Table 1).
Table 1: Factors associated with retention of pharmacists in rural and remote Australia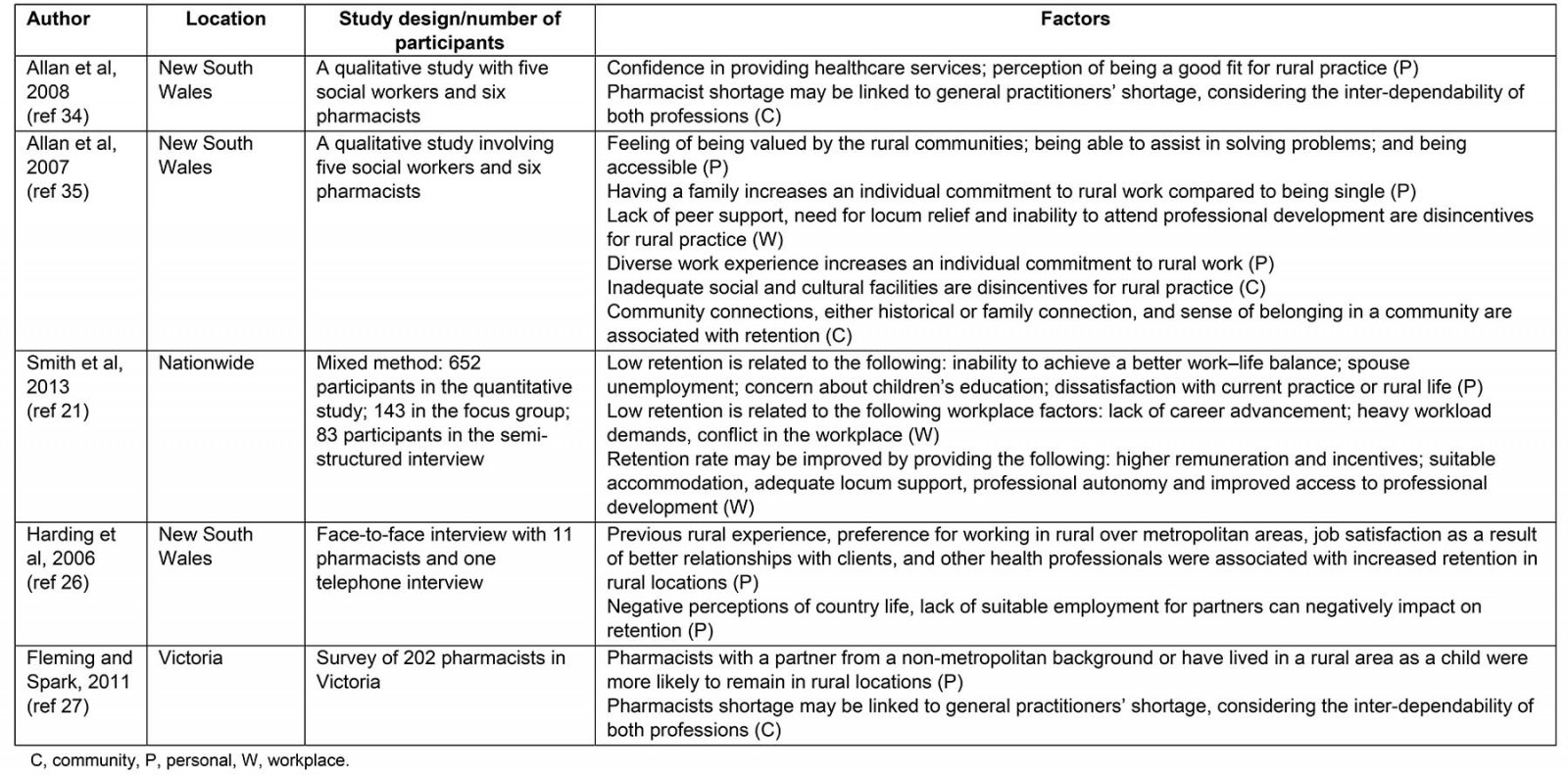
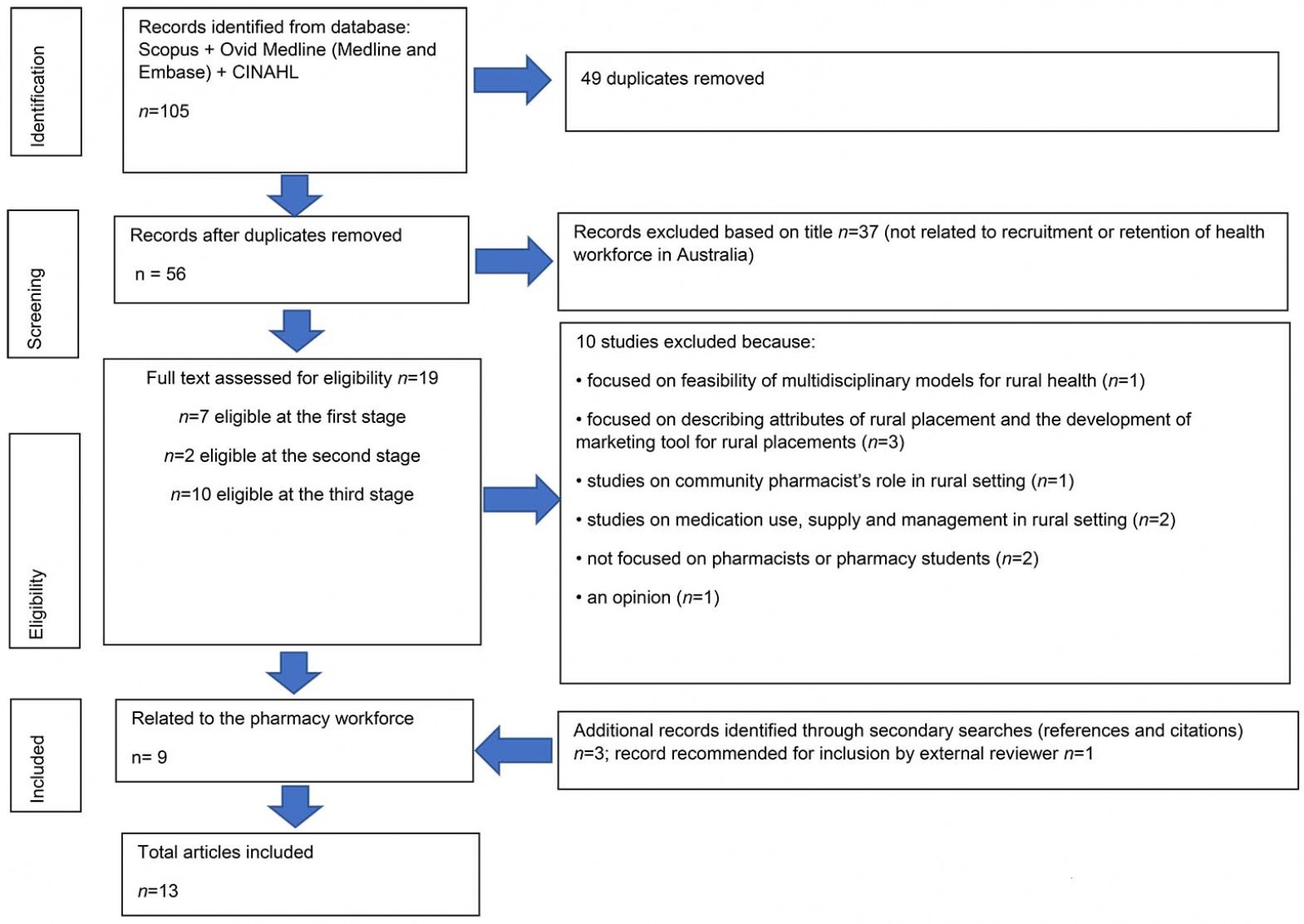 Figure 1: Flow chart of selection process.
Figure 1: Flow chart of selection process.
Preparation for rural pharmacy practice
The literature suggests that rural practice differs significantly from metropolitan practice, and healthcare professionals need to be adequately prepared to cope with the challenges of residing and practising in a rural setting. Several articles identified strategies for increasing the availability of pharmacists in rural areas. Lyle et al surveyed health faculties staff and provided a report on the effort of the University of Sydney in New South Wales to improve the healthcare workforce in rural Australia24. Specifically, strategies that were targeted at the pharmacy profession include enrolment of students from rural backgrounds, availability of support personnel for rural initiatives, extended rural placement and the inclusion of rural content in the teaching curriculum. The authors reported the discipline of pharmacy to be the only program with an established bachelor’s degree curriculum that focuses on rural practice (BPharm (Rural)). The Bachelor of Pharmacy (Rural) curriculum differs from the conventional Bachelor of Pharmacy degree in that students opting for the rural pathway are required to complete a 12-week placement in their fourth year. This is different from the conventional pathway where students only need to engage in 1–2 weeks of placements in their fourth year. The study further reports that, compared to most of the other health programs in the university, the discipline of pharmacy had a higher number of full-time equivalent staff to support rural initiatives, which included attracting and supporting students from a rural origin. However, the BPharm (Rural) program of the University of Sydney has been discontinued and no university in Australia is currently running it.
Similar to the study by Lyle et al, a study by Kemp and Spark reported on a survey of the first four cohorts of BPharm graduates from the Bendigo campus of La Trobe University in Victoria28. The results of the survey showed that those from rural backgrounds were more likely to undertake rural employment and, despite the rural focus of the course, the majority of graduates with metropolitan backgrounds did not proceed to work rurally.
A review conducted by Spiers and Harris in allied health professions, including pharmacy, reported similar findings29. The authors alluded to the research of Taylor et al, which compared the responses of pharmacy students in their first and final years23. In their final year, the proportion of students who signified a positive intention to practise in a rural setting increased to 22%, from 11% reported in their first year. This increase was statistically significant and was reported to be driven by factors including rural background, rural placement and enrolment in the BPharm (Rural) program23. However, no follow-report was found to suggest whether the stated intention to practice in a rural setting culminated in rural practice.
A study by Kirschbaum et al highlighted the importance of rural background and rural placement in influencing student desire to practise in a rural location. In their study, students from rural backgrounds were significantly more likely to desire to work in a rural location compared to those from metropolitan backgrounds30. However, among students who did a rural placement, no difference was observed in the intention to work rurally between students with rural backgrounds and those with metropolitan backgrounds30.
Having a rural background appears to be the most important factor among pharmacists who choose to practise in rural areas, as a qualitative study by Harding et al involving 12 pharmacists also reported26. In their study, many of the pharmacists practising in a rural setting grew up and had always lived in a rural location. The decision to practise in a rural setting could be because pharmacists of rural origin see being ‘rural’ as part of their identity. Moreover, data from the study suggest that economic incentives, including the availability of accommodation and lower overhead business costs associated with a better return on investment, were important considerations for pharmacists before practising in rural and isolated communities26.
The establishment of pharmacy schools in rural areas was mentioned as a strategy for increasing the availability of pharmacists in rural and remote areas in a mixed-methods study by Smith et al21. The study involved 242 participants, including pharmacy students and pharmacy education stakeholders. One of the themes identified from the consultative process is the need for pharmacy schools in rural areas to ensure a continuous supply of rural pharmacist workforce. Participants viewed the establishment of pharmacy schools in rural areas of Victoria, New South Wales and Queensland as a beneficial factor that would support the pharmacy workforce in these locations. This is due to the perception that students from rural areas were more likely to practise in rural communities if they had studied in a pharmacy school in a rural location. Similarly, a survey by Simpson and Wilkinson provided additional evidence on the benefits of rural pharmacy programs22. The investigators described the practice decisions of the first cohort of graduates from Charles Sturt University, a university located in a rural area of New South Wales. The study reported that more than 60% of all pharmacy graduates and about 90% of female graduates had accepted pre-registration placements outside of metropolitan locations.
Despite all the positive features of these strategies, one study by Orpin and Gabriel, which included pharmacy students, reported a contrary observation25. This study was designed as an online survey for first- and final-year medicine, nursing and pharmacy students. The result showed that none of the pharmacy students who recalled participating in rural course work felt that it positively influenced them toward a rural career. Further, only one pharmacy student indicated that their rural placement experience stimulated them towards a rural career.
Recruitment of rural pharmacists
It has been reported that many rural hospitals are not large enough to employ the services of a full-time pharmacist. The use of a sessional pharmacist (contracted part-time employment of a local pharmacist external to the hospital) as a potential recruitment solution was investigated by Tan et al31. In their study, 13 pharmacists, including eight Australian pharmacists, participated in a qualitative interview and described a variety of sessional arrangements operational across New South Wales, South Australia, Queensland and Western Australia. Of the eight sessional positions, two later evolved into full-time positions, three were ongoing sessional positions and three were already discontinued at the time of the interview. Although the mix of responsibilities for a sessional pharmacist varies across settings, dispensing of medication was absent for most sessional pharmacists. Instead, most pharmacists were involved with the quality use of medicines, medication management and clinical governance in their respective settings31.
Factors associated with the retention of healthcare professionals
Australians living in rural and remote areas tend to have poorer health outcomes than their metropolitan counterparts34. One major contributor to this disparity is the health workforce shortage, resulting from a high turnover of health workforce34. A range of factors can impact on the retention of pharmacists after accepting a rural position.
Personal factors: Personal factors have been reported to either encourage pharmacists to stay or leave rural settings. Personal factors that positively influence retention include perception of confidence in their role and being a good fit for rural practice35; feeling valued by communities they serve36; feelings of satisfaction from helping people and being an accessible healthcare provider36; job satisfaction due to better relationships with clients, general practitioners and other healthcare workers; preference for rural practice26; and previous rural experience26. Diverse prior work experience and having a family compared to being single have also been reported to promote retention in rural areas36.
Conversely, negative factors include the inability to achieve a better work–life balance21, absence of suitable employment for spouse21,26 and concerns about children’s education21. Others include dissatisfaction with rural practice or rural life26, feeling professionally isolated26, and negative perceptions of rural life, including underestimation of the facilities available in rural areas26.
Workplace-related factors: The articles retrieved covered several workplace-related factors that can influence the retention of pharmacists. Positive factors include professional autonomy, variety of tasks in a rural setting, use of advanced skills, increased financial incentives, suitable accommodation, adequate locum support and access to professional development, and potential for higher remuneration compared to metropolitan colleagues21. Negative factors are lack of peer support36, high workload, inadequate remuneration, workplace conflict, absence of career advancement, inability to take leave, and limited access to locum relief, professional development and supervision21. To ensure optimal retention of healthcare practitioners in rural areas, Onnis suggested that organisations need to pay considerable attention to the wellbeing of their staff while in the workplace37. To reduce staff turnover, Sutton and Maybery advocated for the continuous development of structures and processes that promote organisational adaptability to the unique circumstances and dispositions of current and potential healthcare professionals38. Such approaches may include more flexible work arrangement, family-friendly employer policies and the use of exit interviews to identify factors influencing staff turnover rate38.
Community factors: The role of community in influencing the retention of pharmacists has been mentioned in the literature. Rural environments have been reported to have certain advantages and disadvantages. For instance, a lack of social and cultural facilities has been reported by community pharmacists as a barrier to rural practice36. Conversely, community connections, historical or family connection and sense of belonging in a community have been positively associated with retention36. This suggests that when rural pharmacists become well integrated into a community, they experience less social isolation and are more likely to continue to practise in that setting. With regards to the viability of community pharmacy practice, the shortage of pharmacists has been linked to a shortage of general practitioners and medical services in some rural and remote communities26,27. It is believed that the prospect of medical services in rural areas would potentially affect the sustainability of pharmacy practice in these areas. A study by Harding et al suggests that pharmacists have been involved in addressing GP shortages in isolated areas26. The study reports that a pharmacist from one rural town was involved in securing financial assistance from the state government to purchase and furnish a house in the town for locum general practitioners and medical students, to recruit these staff26. This was done to increase medical services in the area and to potentially promote the viability of community pharmacy practice26.
Discussion
The present study summarises the recruitment and retention of pharmacists in rural and remote areas. Strategies that have been used include establishment of pharmacy schools in rural areas, inclusion of rural content in pharmacy curriculum, enrolment of students from rural backgrounds, extended rural placement and employment of sessional pharmacists. Factors associated with recruitment and retention were personal, workplace or community factors.
The factors affecting retention of pharmacists are largely similar to those that affect other health professional groups, including the medical workforce3. The effort of the Australian Government toward the retention of the healthcare workforce in rural and isolated communities, however, appears to be disproportionally focused on the medical workforce. This is highlighted by the current initiative tagged Stronger Rural Health Strategy, which details the government’s strategy of building a quality, well-distributed and sustainable health workforce39. Of note, 9 of the 11 strategies are entirely focused on supporting the medical profession39. In contrast, only one initiative (Workforce Incentive Program) involves engaging the services of non-dispensing pharmacists in a general practice setting39.
To overcome the current challenge of providing adequate health services in rural and remote areas, more attention should be paid to pharmacists and other groups of healthcare professionals, and how best they can be effectively utilised. A pragmatic solution is to provide additional training and extended scope of practice for pharmacists, targeted at improving specific areas of healthcare needs in rural, disadvantaged or isolated communities. This approach has been reiterated as part of the blueprint for better utilisation of the pharmacy workforce by 2023 and would potentially improve health outcomes in rural and remote communities5.
While diverse frameworks have been proposed for identifying and addressing workforce retention in rural settings40-42, the conceptualisation and charting of factors into personal, workplace and community factors suggest a holistic approach where graded levels of ecological influence (personal, workplace and community) are considered43. Therefore, to ensure a sustainable rural pharmacist workforce, personal, workplace and community factors should be modified where possible. This would possibly lead to an increase in the pharmacist workforce willing to be employed and retained in rural and remote communities.
Conclusion
The present study described the strategies for increasing the availability and retention of pharmacists in rural and remote areas in Australia. The authors suggest that pharmacists could be utilised more effectively and gain greater job satisfaction by further training in and supporting more expanded roles in the community. Increasing the availability and retention of pharmacists will rely on a mix of personal, workplace and community factors, which need to be well addressed to ensure the long-term retention of this group of health professionals in more disadvantaged and isolated communities.
References
You might also be interested in:
2011 - Farewell Ralph McLean - a quiet contributor to rural health