






Introduction
The relationship between child nutrition and maternal social capital has not been widely explored in developing countries; only a few studies have been made in Peru, Vietnam, Ethiopia and India1,2. There are several ways in which maternal social capital can determine the nutritional status of a child; for example, by increasing the possibility of access to different services such as health care, information and education; by allowing access to assets such as money, provisions and food; and by helping mothers to maintain physical and mental health3.
Another possible mechanism by which maternal social capital can improve a child’s health and nutrition is through social networks1. These networks allow mothers to ‘know more’ because of information transfer (eg where to obtain cheaper resources), to ‘think differently’ because of behavioral influences (eg hygiene and cooking practices), to ‘do things differently’ (eg maintain breastfeeding for longer duration), and to ‘feel differently’ because of emotional support (eg improved mental health).
Two definitions of social capital were used for this study; the first and wider definition describes social capital as a set of intangible attributes present in a society that favor entrepreneurship: trust, reciprocity and social action according to shared norms4. According to Putnam et al, social capital has two key elements: structural social capital and cognitive social capital4. The first reflects the links and connections that people have in a community by being active and participating in internal activities. The second reflects the sense of being part of the community by addressing the confidence in the community, social cohesion, common local guidelines, and recognition of reciprocity2.
The second and more recent definition visualizes social capital as informal relationships of trust and cooperation (family, neighbors, colleagues), formal associativity in organizations of different types, and the institutional framework (rules and values) of a society that fosters or inhibits relationships of trust and civic commitment5.
The hypothesis used for this study was that maternal social capital can be effective in improving a child’s nutrition, especially when physical and human capital are uncommon. Thus, this study aimed to determine the social capital of mothers with young children and to determine the association between maternal social capital and their children’s nutritional status. This study was conducted in San Isidro, a parish on the Ecuadorian coast that suffered the impact of an earthquake in 2016. Therefore, questions about social capital include receiving help after the earthquake.
Methods
Study area and sample size
A cross-sectional study was conducted in San Isidro, a rural parish located in the province of Manabí, on the coast of Ecuador, in September 2017. San Isidro parish has 10,987 inhabitants (35.7% urban and 64.3% rural) and its area is 296 km2. The climate is tropical, dry and humid, and the average temperature fluctuates between 24°C and 26°C. The economy of the parish is based on agricultural and livestock activities6.
The sample size was calculated by using an estimated prevalence rate of chronic malnutrition of 24.7% in rural coastal children of Ecuador, a 95% confidence interval (CI), and a precision of 5.0% and 10% for missing data. The minimum sample size required was calculated to be 314 children aged 0–59 months6.
The study was conducted at public daycare centers and schools. For all procedures performed on children, the presence of the mother was required. Children with diseases or conditions that have an influence on nutritional status were excluded from the study.
Questionnaires
The questionnaire for this survey consisted of three sections. The first section was adapted from the Multiple Indicator Cluster Survey (UNICEF)7 and the National Health and Nutrition Survey (ENSANUT-2012), developed by the Ministry of Health of Ecuador and the National Institute for Statistics and Census8. It included questions about demographics and socioeconomic status, maternal and paternal information, health, and nutrition of children, including anthropometric measurements.
The second section was based on the Latin American and Caribbean Scale for Food Security (Escala Latinoamericana y Caribeña de Seguridad Alimentaria – ELCSA)9. It included questions about food security.
The third section, based on the Social Capital Assessment Tool of the World Bank10, addressed information concerning the family’s social capital.
The questionnaire was adapted and validated to San Isidro’s culture to ensure its appropriateness. Trained nutrition students collected data via personal interviews directed to the children’s primary caregivers, usually the mothers.
Anthropometrics and blood samples
Researchers observed the recommended technical standards and criteria throughout all steps of the anthropometric evaluation. Children’s and mothers’ weights and heights were measured as described elsewhere6. In summary, weight was measured with portable electronic microscales (ADE, model M320600, Hamburg, Germany), height was measured with a portable stadiometer (SECA model SECA 213, Hamburg, Germany), and length was measured by using a length board (ADE model MZ10027-1, Hamburg, Germany). The precision of the instruments was 100 g for weight and 0.1 cm for length/height). Z-scores for length-for-age, weight-for-age and weight-for-length were calculated by using the WHO 2006 Child Growth Standards for children under 5 years11.
A sample of venous blood (3 mL) was collected from each child and hemoglobin values were determined with a spectrophotometer.
Variable description
The dependent variable ‘chronic malnutrition’ or stunting was determined by the height-for-age Z-score ≤2 standard deviations11. Anemia was defined as a blood hemoglobin level of <110 g/L for children 6–59 months of age at sea level12.
The questions for cognitive and structural social capital considered the relationships that the family, particularly the mother, had with other members in the community (eg ‘After the earthquake emergency, were you helped by community members or did you help them? – Yes/No’, ‘In an emergency, were you helped by friends and family? – Yes/No’ ‘Money borrowed? – Yes/No’), their participation in community groups (eg ‘Mother being part of a community organization – Yes/No’, ‘Mother takes part in community activities – Yes/No’), and their feeling of belonging (eg ‘Will you live several more years in your community? – Yes/No’, ‘Do you like your community? – Yes/No’).
Covariates for this study were children’s ages, mother’s age, number of children, maternal education level, family income and food security. These covariates are directly and critically related to children’s nutritional and health status. Maternal education is expected to improve a child’s nutritional status by changing preferences and resource allocations, and by improving childcare practices13-15. A higher family income is related to an improved children’s nutritional status, probably because of access to higher quantities of nutritious and tasty foods12-14. It also relates to the access to better health services16-18. The number of children in a household was considered to be a proxy of family size, the reason being that number of children is related to their nutritional status because of the ‘competition’ with other children for attention, care, food, and sometimes scarce resources19-21.
Statistical procedure
Bivariate analysis and multivariate logistic regression models were used to measure the association between social capital and dependent variables (anemia and chronic malnutrition), using Poisson regression models (prevalence ratio (PR) and 95%CI). The multivariate models were adjusted by covariates: mother’s age at childbirth, child’s age, family income, number of children in the household, and food insecurity. Variables that were significant (p<0.20) in the bivariate analysis were maintained for the multivariate model. Only significant variables (p<0.05) were maintained in the final model. The OpenClinica software v.3.7 (https://www.openclinica.com) was used in data entry and STATA v15.0 (StataCorp LLC, Texas, USA) was used for statistical analysis.
Ethics approval
This research involved human participants. Mothers or guardians of the children signed a written informed consent to participate in this study. Illiterate mothers consented by their thumbprint after verbal consent. The Institutional Review Board from the Pontifical Catholic University of Ecuador (protocol number CEISH-297-2017) and from the Ministry of Public Health of Ecuador (protocol number MSPCURI000216-3-etapa 1) approved the protocol.
Results
A total of 246 children for anemia and 282 for chronic malnutrition were included in the multivariate analysis. The prevalence of anemia and chronic malnutrition was 15.0% and 12.8%, respectively.
Table 1 shows characteristics of the sample. Children’s ages ranged from 1 to 59 months and the most frequent age group was 49–59 months (35.4% for the anemia sample and 35.1% for the chronic malnutrition sample). The most frequent group for mother’s age at child’s birth was 20–25 years (32.9% for anemia and 34.7% for chronic malnutrition). Forty percent of mothers were illiterate or had only finished primary education.
Most families had one or two children (61.8% for anemia and 63.1% for chronic malnutrition). Considering the family income per month, 57.3% in the anemia sample and 54.6% in the chronic malnutrition sample earned from US$80.10 to US$300 (less than the 2017 minimum wage of US$375).
In relation to structural social capital, after the 7.9-magnitude earthquake in April 2016, 64.5% of the anemia sample and 63.8% of the chronic malnutrition sample received and provided help. A low percentage of mothers were part of a community organization (18.7% for anemia and 18.1% for chronic malnutrition). Approximately 40% of mothers participated in community activities and 30% of mothers had borrowed money in both samples.
In cognitive social capital analysis, a higher proportion of mothers (96.7% for anemia sample and 95.7% for chronic malnutrition) liked their community, and were willing to live more years in that community (92.3% for anemia and 90.4% for chronic malnutrition).
Finally, descriptive analysis of food security variables showed that more than half of households were worried about the scarcity of food in the previous 3 months (62.6% for anemia and 62.1% for chronic malnutrition). In addition, approximately 20% of households reported that they were out of food because of a lack of money in the previous 3 months and were forced to reduce the quantity of food for someone aged less than 18 years in the previous 3 months (Table 1).
Social capital and anemia
The prevalence of anemia was higher in children whose mothers were part of a community organization than in children whose mothers were not (26.1% vs 12.5%, p=0.021) (Fig1). In bivariate (PR 2.02, 95%CI 1.13–3.60) and multivariate analysis (PR 1.90, 95%CI 1.04–3.48), a mother being part of a community organization was positively associated with anemia (Tables 2,3). The other variables were not significantly associated with anemia in bivariate or multivariate analysis (Tables 2,3).
Social capital and chronic malnutrition
The prevalence of chronic malnutrition was lower in children whose mothers had borrowed money than in children whose mothers had not (8.1% vs 14.8%, p=0.049) (Fig2). In addition, a lower prevalence of chronic malnutrition was observed in children from households who were helped after the 7.9-magnitude earthquake than in children whose families did not receive help (8.3% vs 20.6%, p=0.003).
In multivariate analyses, receiving help after the earthquake was associated with a lower prevalence of chronic malnutrition (PR 0.52, 95%CI 0.28–0.97). In addition, children whose mothers had borrowed money were less likely to have chronic malnutrition (PR 0.43, 95%CI 0.20–0.90) than children whose mothers did not (Table 3).
Table 1: Characteristics of the sample, San Isidro, Manabí, Ecuador, 2017 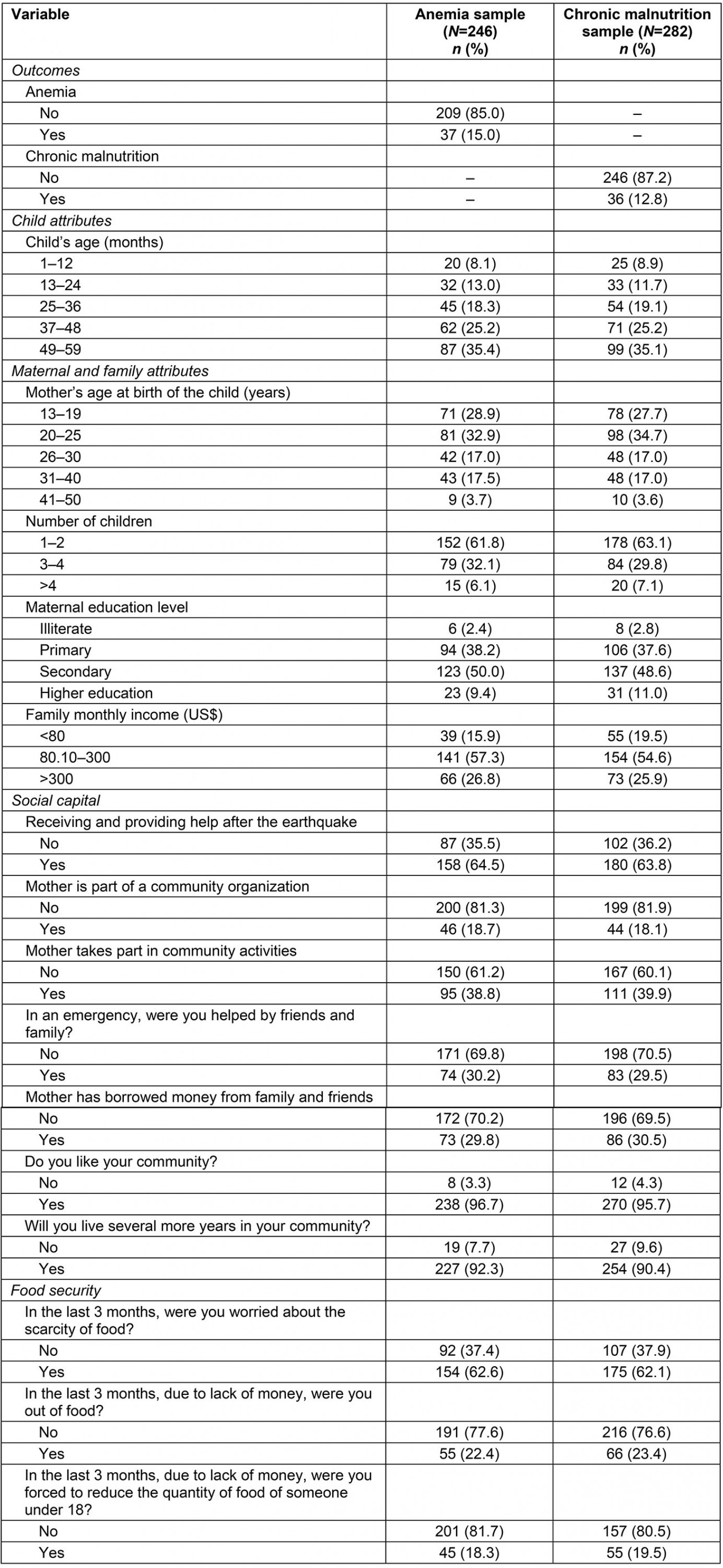
Table 2: Bivariate analysis between social capital, anemia and chronic malnutrition adjusted by confounding variables, San Isidro, Manabí, Ecuador, 2017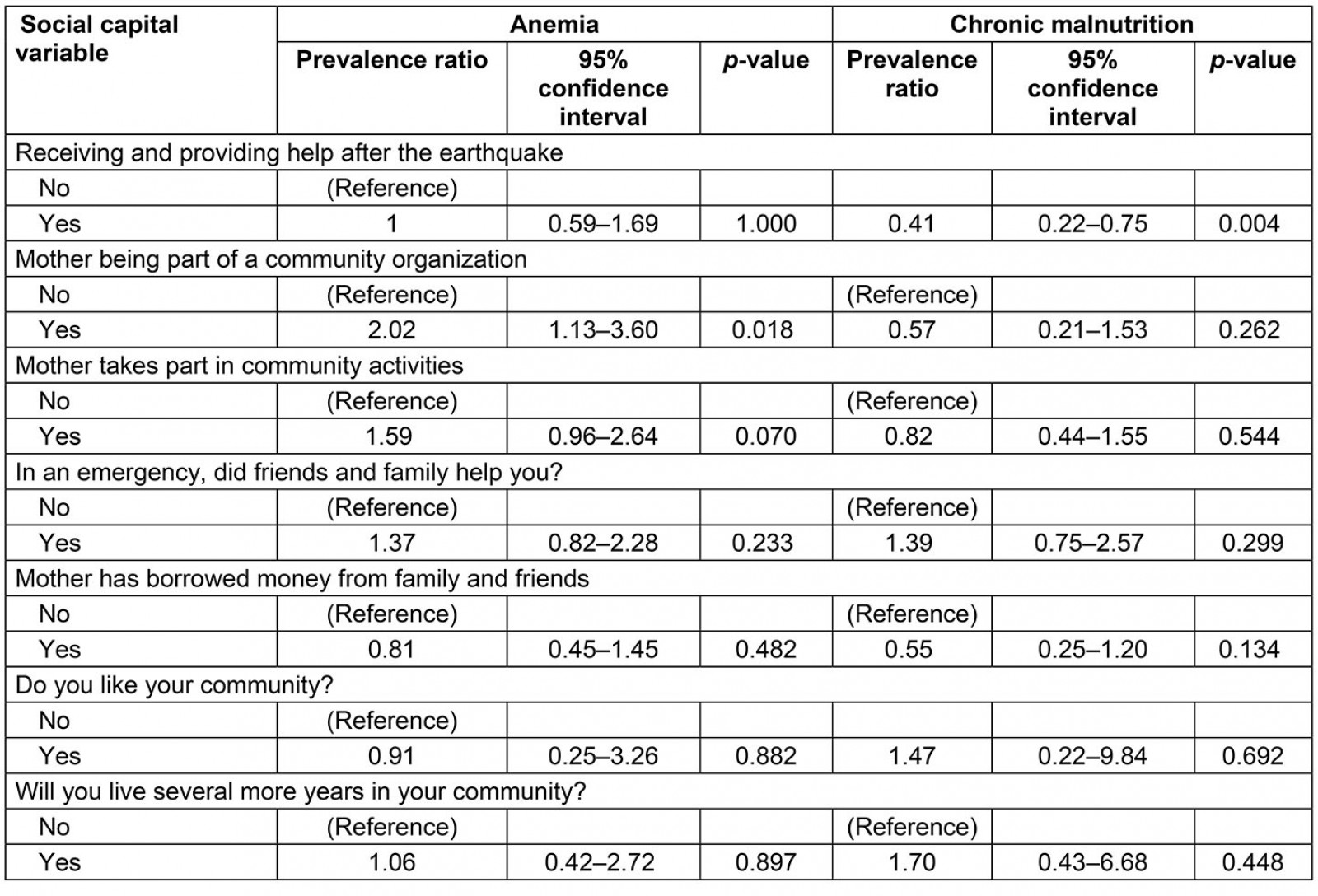
Table 3: Multivariate analysis (final models) for the association between social capital, anemia and chronic malnutrition adjusted by confounding variables, San Isidro, Manabí, Ecuador, 2017†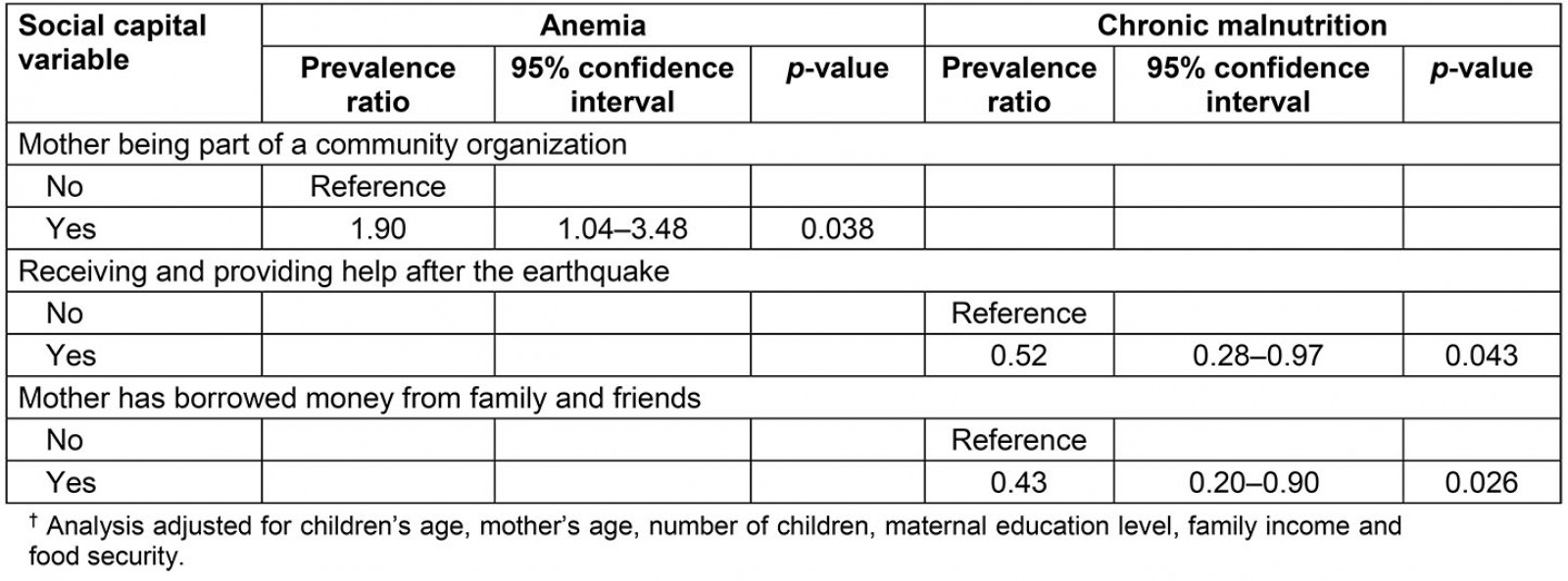
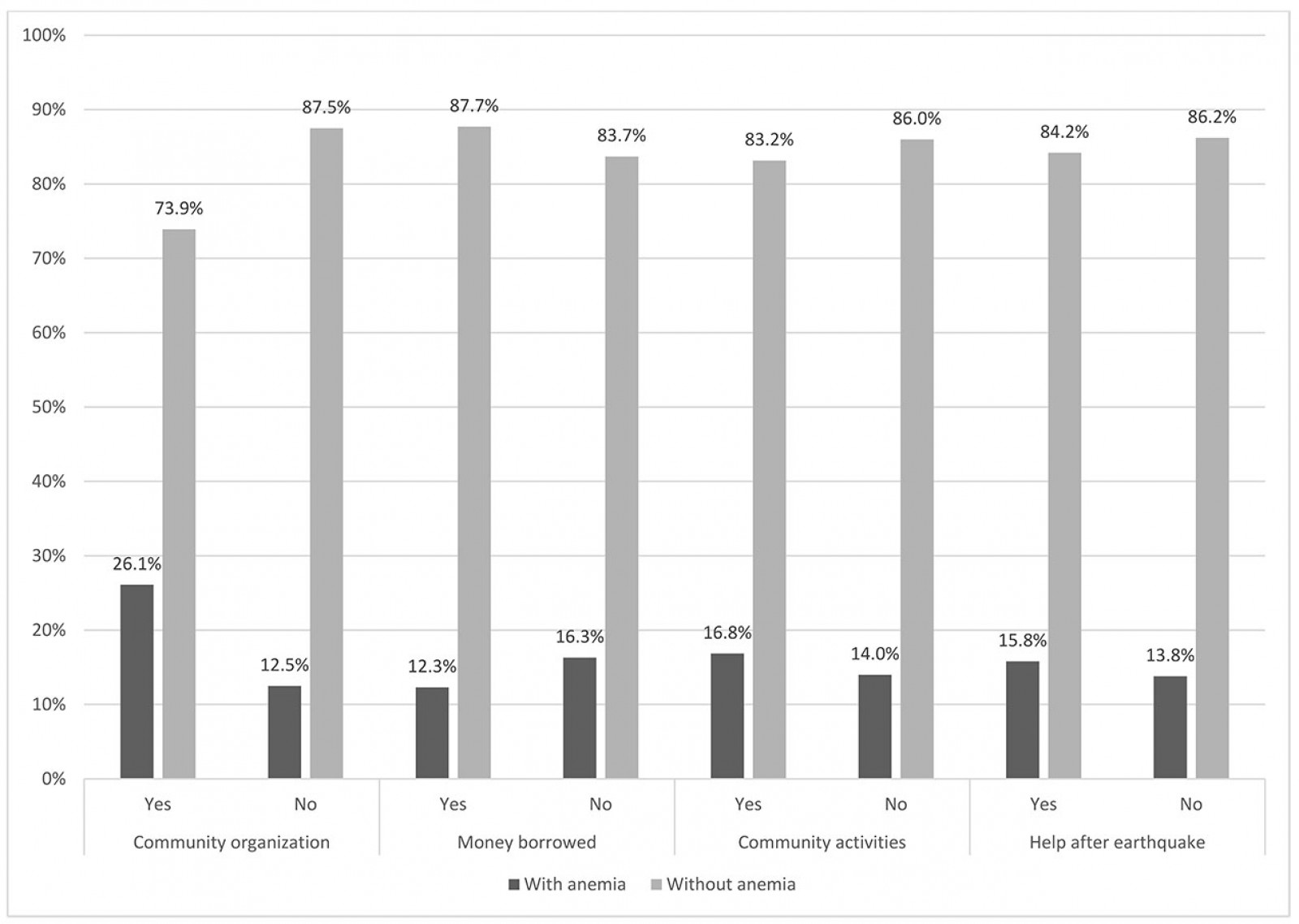 Figure 1: Social capital variables in children with and without anemia, San Isidro, Manabí, Ecuador, 2017 (n=246).
Figure 1: Social capital variables in children with and without anemia, San Isidro, Manabí, Ecuador, 2017 (n=246).
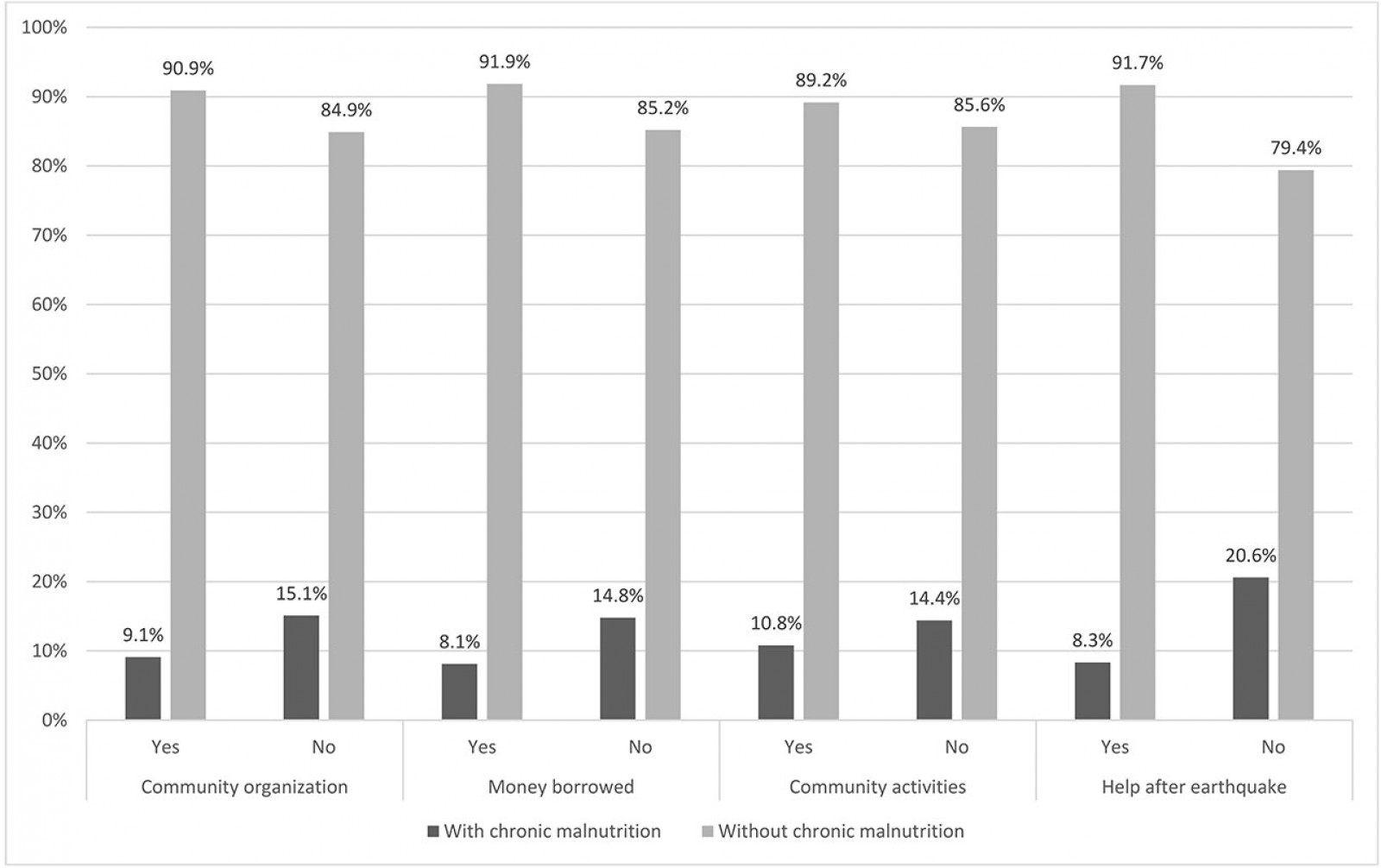 Figure 2: Social capital variables in children with and without chronic malnutrition, San Isidro, Manabí, Ecuador, 2017 (n=282).
Figure 2: Social capital variables in children with and without chronic malnutrition, San Isidro, Manabí, Ecuador, 2017 (n=282).
Discussion
This study provides data on the relationship between a mother’s social capital and their child’s nutritional status (anemia and chronic malnutrition). The reciprocity relationships observed in the support received by the community after the 2016 earthquake and having borrowed money from family, friends or community members were protective factors for chronic malnutrition. However, being part of a community organization increased the prevalence of anemia.
After the multivariable analysis, the results show that receiving help from community members or helping them after the earthquake (used as a proxy for structural social capital and bonding social capital) showed a protective effect on chronic malnutrition. By helping people who were affected by the earthquake, some resources may have been directed to address the needs of children of the households before other matters. The fact that a mother borrowed money (also used as a proxy for structural social capital) may have been a demonstration of the community solidarity and was shown to have a protective effect on the nutritional status of a child. This money may have helped mothers to access more resources for food, health services, and hygiene supplies.
Similarly, some studies have shown a protective effect of social capital on the nutritional status of children. One study in Peru analyzed the relationship between maternal social capital and the nutritional status of children. It found a positive relationship between maternal structural social capital and a child’s nutritional status. A child whose mother was part of a community group was 1.1 cm taller than children whose mothers were not part of a community group2.
Likewise, in rural areas in Laguna, Philippines, children whose mothers had higher maternal social capital scores (being active members of organizations, attended social events, having high network density) had a lower probability of a poor nutritional status, regardless of the community they belonged to. Additionally, weight-for-age and height-for-age were found to have a significant association with maternal social capital in rural areas22. A study in rural Ethiopia has shown that support from two or more individuals was associated with meeting a minimum level of dietary diversity (OR 5.2, 95%CI 1.32–20.40)23.
In the present study, some contradictions were found with the hypothesis that maternal social capital can be related to a child’s nutrition improvements. The results suggest that children whose mothers participate in community organizations are more likely to have anemia. Studies in India, Peru, Vietnam and Ethiopia have shown that maternal group membership was not related with either height or weight of children even after adjusting the model for confounding variables1. Additionally, children whose mothers were involved in citizenship activities showed lower height-for-age Z-scores in the India study, and lower weight-for-age Z-scores in the Ethiopian study1. No association between maternal cognitive social capital and child nutritional status was evident in the study in Peru1. De Silva and Harpham suggested that these results should be cautiously interpreted from cross-sectional data1. Further longitudinal research will need to be undertaken because it is not known if mothers were participating in community groups because their children were not growing properly, or if children were suffering because of the activities of mothers1. Stress caused by community participation, added to that caused by a mother’s productive and reproductive roles, could have had a negative impact on the mother’s mental health1 and affected the nutritional status of children.
Regarding the relationship between frequency of meals of children and maternal social capital in Ethiopia, being a member of a community group (OR 0.35, 95%CI 0.20–0.59) or having one type of citizenship activity (OR 0.39, 95%CI 0.20–0.76) showed decreased odds of meeting the minimum meal frequency for children19. The authors of that study hypothesized that this inverse relationship could have been due to the lack of trust in community members, and mainly associated with cognitive social capital. Additionally, Coleman stated that social capital could negatively influence innovation when an individual adheres to group norms24. Therefore, mothers with high social capital would be convinced and influenced by the social norms of that community, some of which may have not been adequate for children’s nutrition24. It is likely that these studies underestimated the influence of social capital because they did not distinguish between the different types of social capital (bonding and bridging), which could be acting in opposite directions25.
The results of the present study suggest that social capital appears to work in a non-intuitive way. Bonding social capital, which generally refers to ties between family members and friends, had a positive impact on child nutrition. There is evidence to show that bonding social capital is positively related to overall improved healthcare access and use across countries26. However, this role may depend on the norms or beliefs of members within the network26. At the same time, bridging social capital, especially when it entails participation in organizations, did not prevent children from having nutritional problems. Bridging social capital can potentially improve child health outcomes by making more information available about health, local services, and ways to access them27. However, if a community lacks or has limited access to safe water, transportation, and health services, then bridging organizations are able to do little by themselves to affect nutritional outcomes of children.
Most research has focused on the association between a mother’s social capital and child nutrition, whereas research on the relationship between a father’s social capital and child undernutrition in developing countries is sparse. In recent years, the importance of a father’s role in child nutrition has been recognized28. For instance, a study found that a father’s financial contributions to child nutrition and health care enhanced their children’s nutritional status29. Similarly, the nutritional condition of Mexican American children was favorably connected with the father’s engagement in feeding practices30.
This study is a first approximation of the relationship between social capital in mothers and nutrition of their children in a rural area of Ecuador. Moreover, it can be the beginning in the development of similar studies that could address the effect of social capital on health outcomes. However, results from this study may lack external validity because of the limited study area (a single rural parish in coastal Ecuador affected by an earthquake). Other weaknesses are the sample size for some categories, which may influence the results of the associations, and the cross-sectional study design, which is not the best for causation analysis between social capital and anemia or chronic malnutrition. It is highly recommended that information be gathered in several points in time for further causation analysis. Finally, this study did not analyze the relationship between social capital and parenting practices (ie breastfeeding and care practices), variables that could influence the results of the association between social capital and anemia or chronic malnutrition on children.
Conclusion
Maternal social capital and the nutritional status of their children in a coastal rural community of Ecuador seems to be positively related. Structural social capital or bonding social capital (mother had borrowed money from family or friends, and the reciprocity relationships observed in the support received by the community after the 2016 earthquake) had a protective effect on chronic malnutrition. This study emphasizes the importance of improving bonding social capital in community intervention programs. The study also found that bridging social capital (mother’s participation in community organizations) was associated with a higher prevalence of anemia and had no impact on chronic malnutrition. These mixed results highlight the need for further studies focused on the different types of social capital and how they affect health in deprived areas.
Acknowledgements
The authors thank the Parish Government of San Isidro, District of Education of San Isidro, Zonal Coordination No. 4 of the Ministry of Economic and Social Inclusion, and schools and childcare centers of San Isidro, for providing the facilities to conduct surveys with the parents and their children included in this study. The researchers also thank the congregation Hermanas Hijas del Amor Divino, San Isidro Health Center’s director (Daniel Guerrero), primary healthcare technicians (Johanna Macias, Clelia Arteaga, Cecibel Velasco) and the Education Circuit Coordinator from San Isidro (Liliana Moncayo) for supporting the data collection. Data management oversight was provided by Cesar A. Yumiseva and Alberto Larrea from the Center for Research on Health in Latin America at Pontificia Universidad Católica del Ecuador (PUCE).