

Introduction
Chagas disease (CD) is caused by the protozoan parasite Trypanosoma cruzi (T. cruzi)1. CD affects 6 to 7 million people worldwide, and 30 000 new cases are reported each year2. The disease is endemic to 21 Latin American countries; however, in recent decades CD has spread globally to non-endemic areas such as Canada, the USA, Europe, Australia and Japan3. The most common way to be infected with T. cruzi is through the feces of certain species of triatomine bugs, also called ‘kissing bugs’. Transmission to humans is associated with triatomine species adapted to live inside houses in rural areas. These insects hide during the day in the cracks of walls and roofs of precariously constructed houses and emerge at night to feed4-7. Inadequate housing, and poor vector control within and around houses, have been identified as a risk factor for triatomine colonization8. Thus, prevention programs often focus on the interruption of household transmission as well as educational programs1,9.
In South America, CD is a major health problem in several regions, causing more than 12 000 deaths per annum, and placing more than 5 million people at risk of acquiring the disease3. Although interventions in Brazil, Argentina, Ecuador and Colombia have been successfully implemented and the risk of transmission dramatically reduced, all vector control programs face limitations and challenges10-12. For example, knowledge assessments from Peru, Mexico and Bolivia have found low levels of awareness of CD and a lack of knowledge about its transmission, symptoms or causative agent12,13. In high-risk communities, this disconnect between triatomines and CD is also associated with low interest in prevention of CD and substantial underestimation of the risk of CD. For instance, in southern regions of Ecuador, triatomine infestations of houses reached up to 48% and are often associated with chickens and guinea pigs being kept inside the house14. Thus, developing educational programs around CD transmission (vector–parasite), risk and prevention may be needed to improve CD prevention programs.
New and alternative strategies such as holistic strategies that include health promotion focusing on improvement of living environment and system-based health promotions to prevent CD have been implemented in places such as Ecuador since 201312. In Ecuador the incidence of CD is high. The Ecuadorian Ministry of Health estimates 36 new cases per 10 000 inhabitants per year, resulting in 4400 new cases each year15. The southern province of Loja in Ecuador is particularly vulnerable to this disease. Loja province has the highest poverty in the country, and a higher rate of inadequate housing environments has led to bug infestation rates of up to 48% in domiciliary units within the province6,7,14. Strategies to combat CD in the country mainly focus on active searches for triatomines and insecticide-based spraying in homes, as well as educational programs for CD prevention14. Despite control efforts implemented in the country, CD remains highly prevalent among those aged over 5 years, while 25% of the total Ecuadorian population remains at risk15.
This study seeks to assess young people’s knowledge and attitudes to CD in the three communities with previous intervention programs by the Healthy Living Initiative (HLI)16. Primarily, the initiative focuses on CD prevention through holistic health promotion7. Promotion of healthy practices includes educational programs directed toward youth to affirm cultural and social norms that support health and prevent CD transmission16. Since 2013, the HLI has implemented intervention programs directed toward youth and children with the purpose of implementing community-based research for CD prevention and control. For instance, entertainment education has been proven to serve as a powerful intervention among children in the studied communities17. Previous educational programs toward youth also included participatory research about Chagas prevention, participatory sketching, storytelling projects to promote awareness and song development to prevent CD18,19. In the present study, secondary school children were reached in the community that had previously participated in educational programs from the HLI initiative since 2013. These secondary school students can serve as important informants for identifying gaps and successes from educational programs. The following two core research questions were asked:
- What is the current state of knowledge about Chagas disease among youth in rural communities of southern Ecuador?
- What components of intervention programs do youth identify as motivating to participate in efforts to control CD?
Answering these questions is essential for the improvement of youth-directed intervention programs that have the goal to prevent CD transmission. They may also be transferable to programs that seek to improve health globally.
Methods
Study area
This study was conducted in Loja province in southern Ecuador (Fig1). Loja province, and specifically the southern mountains, is a region that experiences high rates of CD, endemic poverty and low access to human services in comparison to the rest of the country4,17. All participants were recruited in Cariamanga, a city of approximately 14 000 residents. Cariamanga serves as an economic, health and educational center for residents of rural communities from across Calvas county. Youth between the ages of 14 and 18 years come to Cariamanga because it has secondary schools that serve the 840 km2 county. These nearby communities face precarious socioeconomic conditions and have limited access to sanitation, health and education services20. Three of these communities – Bellamaria, Chaquizhca and Guara – have experienced very high rates of triatomine infestation and were identified for economic, educational and sociocultural intervention by the HLI nearly two decades ago4,6. Youth from these communities come to Cariamanga after finishing primary school if their families can afford the transportation costs, boarding costs and loss of labor on their subsistence farms.
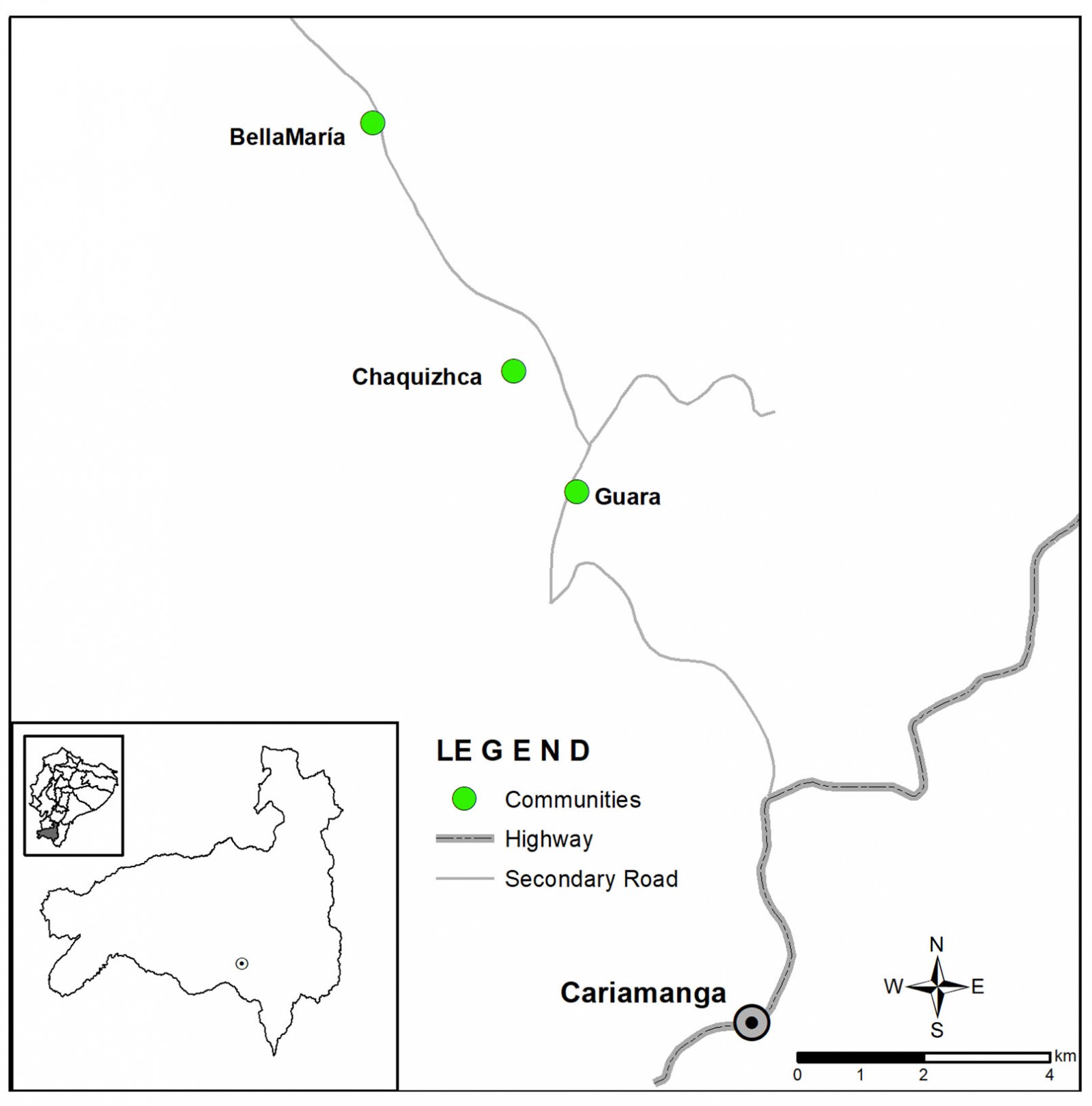 Figure 1: Map of the study area. Cariamanga, the county capital, is shown in relation to the locations of the three rural communities in which study participants lived.
Figure 1: Map of the study area. Cariamanga, the county capital, is shown in relation to the locations of the three rural communities in which study participants lived.
Participants
Youth from Bellamaria, Chaquizhca and Guara attending secondary school in summer term 2018 in Cariamanga were invited to participate. Youth were recruited for two main reasons. First, adult perspectives on Chagas disease in these three communities have been accessed several times in the past16,21,22 and interviewing the youth could provide additional perspectives. Second, although the authors have reported on various projects carried out with youth in these three communities18,23, these previous projects have not reported on how these interventions with the children may have a potential longer term influence on understandings of CD. To be included, a youth had to be aged between 14 and 18 years, born and raised in one of the three communities, and have participated in HLI programs at their primary school in 2013 or 2014. Secondary students who did not meet all three criteria were excluded from the study. School records indicated that there were 39 students from the three communities registered at the secondary school in Cariamanga. However, only 17 were in attendance during the study period owing to absenteeism for lack of funds for transportation, need to work on the family farm, illness, or other reasons. Three potential participants, after an initial screening for the three criteria, did not meet all inclusion criteria. Fourteen adolescents were included. All 14 participants (eight females and six males) lived in Cariamanga during the week to attend secondary school, returning home each weekend.
Study design, process and procedures
A descriptive, qualitative approach using individual interviews was used. Interviews were conducted in Spanish over 2 days in a private room by a member of the research team who is a native speaker from Ecuador. A semi-structured interview guide was used. Questions were structured in a way that young people were able to comment on CD and triatomine bugs, their knowledge about the disease and their views of health intervention programs. All questions in the interview guide were developed in consultation with public health scholars, epidemiologists and employees of the Equadorian Ministry of Health to ensure that they addressed topics relevant to the transmission of Chagas disease. The questions were also reviewed by educators to ensure that the questions were age- and culturally appropriate. Each interview lasted between 20 and 30 minutes. Interviews were recorded on a digital recorder. Participants were asked not to discuss the topic or questions with other participants until all interviews had been completed.
Interviews were transcribed in Spanish using the transcribing software Transcribe Wreally (https://transcribe.wreally.com). After transcripts were reviewed for accuracy by comparing the transcript to the audio-recording, they were analyzed using principles of thematic analysis24,25 using ATLAS-TI qualitative data analysis software v7.1.0 (https://atlasti.com). Following Glaser’s recommendations for emergent thematic analysis26, constructs used to guide the HLI were employed as a sensitizing framework. Using the concepts of vectors, prevention, risk and intervention as the primary sensitizing concepts, participant talk was sorted into preliminary themes. This approach allows for theoretically informed categorization but does not force data into these categories, as additional ways of sorting and categorizing these themes was allowed to emerge.
Coding was performed by two independent reviewers. One coder conducted the interviews, and the other coder was not associated with data collection but was familiar with the work. If a new theme appeared to emerge for a coder they discussed it with the other coder until consensus that a new theme had emerged. Coders, in sorting through participant talk, placed statements into a code family, and if there were discrepancies between coders they discussed the categorization until consensus was reached. The coders then revisited these code families to sort them into categories and subcategories. After finalizing the categories, the coders then named the themes to reflect the constructs contained within those themes. Finally, the articulated codes, categories and themes were fit with larger meaning structures for practical change.
Ethics approval
Written informed consent from each youth was obtained from their parents or legal guardians. Written consent was obtained during home visits as part of other research conducted in the communities during the summer. Each parent or guardian and each participant was given a copy of the informed consent or assent for future reference. The study was approved by the Institutional Review Board at Ohio University (18-X-120) and the Ethics Committee at the partner university in Ecuador (2018-36-EO).
Results
Two main categories were identified for how youth in Cariamanga articulate their understandings of CD and related topics. These categories are (1) determining the state of scientific, actionable knowledge related to CD among youth and (2) exploring ways in which youth can become agents of change for control of vectors associated with CD. Within each category, subcategories were articulated. A summary of themes, categories and codes is provided in Table 1.
Table 1: Summary of themes, categories and subcategories of the coding process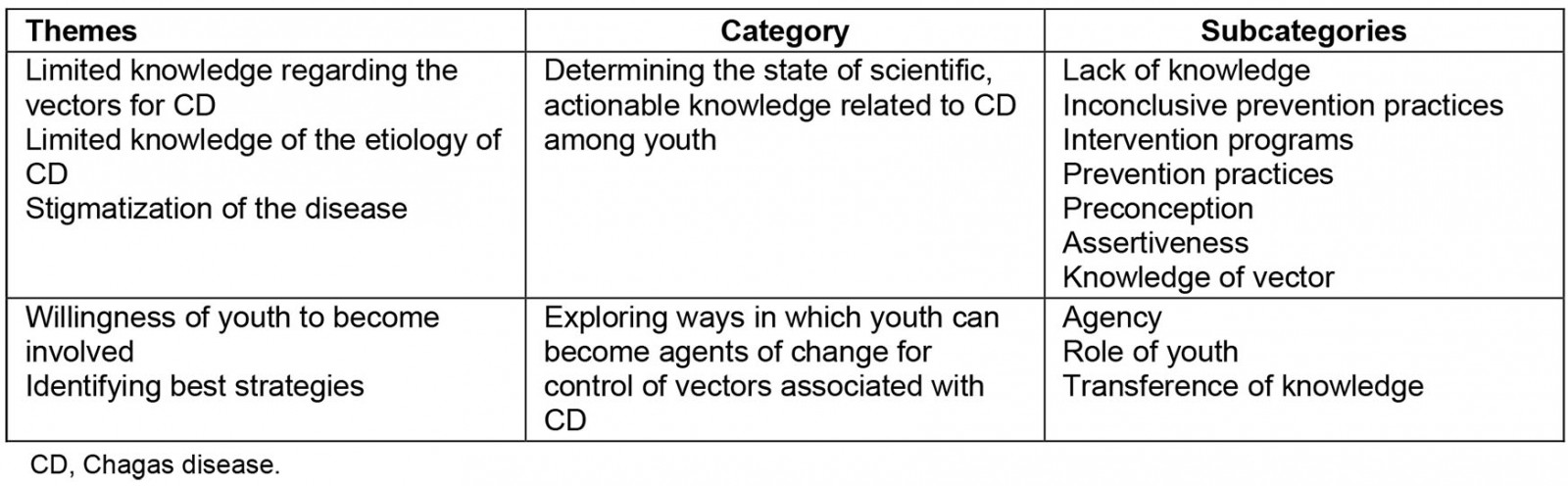
State of scientific, actionable knowledge
The first category, ‘determining the state of scientific, actionable knowledge’, comprised three themes: limited knowledge regarding the vectors for CD, limited knowledge of the etiology of CD, and stigma associated with CD. Each theme represents an opportunity for better scientific communication toward the prevention of CD.
Limited knowledge related to CD vectors: Overall, contradictions were found between the knowledge of the vector and its relationship to CD. For example, participants showed high concerns about having a ‘deadly disease’ or a ‘serious disease’. Surprisingly, this disease was not identified as CD. However, while participants were aware that having the chinchorro (the local name used to identify the triatomine) living inside the house was risky in some way, they did not connect the presence of the bug with the risk of contracting CD. For instance, a 15-year-old male from Bellamaria said he was not afraid of the bug ‘because they are too small, and they can’t do anything’. Similarly, a 17-year-old participant said, ‘I’m not afraid, I mean they don’t look aggressive, they are small, harmless, but when you sleep … that’s a different thing, it’s a danger’. In contrast, a 17-year-old female from Bellamaria said: ‘I usually run when I see one … because the disease they can transmit’, but she did not name the ‘disease’.
These contradictory reactions led to one of the study’s major findings associated with prevention practices. It was found that prevention practices were not correctly applied or followed. For example, a 14-year-old boy from Bellamaria described how he reacted after he sees a chinchorro inside the house: ‘I grab a plastic bag, I collect the 'chinchorro' and put it inside a flask … later, I throw it away and bury it’. A 16-year-old participant also mentioned that she killed the bug with a shoe or anything in hand. Although these actions kill the bug, they are dangerous because a person could come in contact with the feces and get infected with the parasite T. cruzi. Not following the proper protocol represents a risk of contamination to the population. Good prevention practices include collecting the bug safely using a bag, placing the kissing bug in a flask and reporting to local authorities. Based on that data, the study identified a lack of proper implementation prevention practices among participants as representing a major gap in knowledge regarding CD.
Limited knowledge about the dangers of finding triatomines inside the house and how the disease is transmitted were also identified. For example, even though participants were aware that having animals inside the house could attract triatomines, the presence of dogs, guinea pigs, and chickens co-habiting with the family were often mentioned. This is a problematic because domestic animals can serve as intermediate hosts for the T. cruzi parasite27. Triatomines can colonize chicken nests, guinea pig pens, rodent nests and places where domestic animals live, and serve as a reservoir for parasite transmission27. In the specific area of the present study, it is not uncommon for animals such as dogs, chickens or guinea pigs to be kept inside the house to protect them from predators17. Such relocation results in an increased risk of CD transmission. However, even though participants were aware of the presence of kissing bugs, they still did not know that the insects can transmit the parasite that causes CD.
Limited knowledge regarding the etiology of CD: The authors found an unfamiliarity among participants with the parasite (T. cruzi) that causes the disease. Youth indicated incorrect transmission pathways, creating a complex chain of scientific inaccuracies that make it difficult to address vector control among the population. The disease was often confused with a virus among participants. For example, when a 15-year-old participant from Bellamaria referred to CD as a virus:
… the ‘chinchorro’ and depending on the ‘chinchorro’, they often bite us and there is that disease … those viruses that they have can go to the body and give us diseases.
A 15-year-old participant explained Chagas:
… from what I understand … it’s a virus, it is transmitted through an insect that when you sleep … it bites you in the way it can infect you and then … it affects more and more … from there you have some symptom like fever …
Misinformation and stigmatization about contact from person to person through false routes such as kissing or touching were also mentioned. For example, some youth believed CD is transmitted through kissing and person-to-person infection (like the common cold). For instance, a 16-year-old female from Bellamaria mentioned:
... if one person has the disease and we imagine this disease goes to another person, they don’t get contagious just because of the bug bites you, but because it transmits through physical contact … and if that person touches another one it can contaminate all the population … so, yes, I think is alarming.
The fact that participants mentioned person-to-person physical contact as a route of transmission could be associated with the limited knowledge of the participants regarding Chagas disease transmission. Morover, when participants were asked about the symptoms and treatment commonly associated with CD, several gaps in knowledge were identified. For instance, participants often confused the chronic- and acute-phase symptoms, as they often refer to a ‘deathly disease’. However, they seem to believe that home remedies can be used to treat the symptoms. Misinformation between the two phases (chronic versus acute phase) of CD was clearly identified. A participant mentioned:
… if it’s not that bad … you can treat them with a home remedy like we always do here. Well in my house we do it like this … when we have some kind of disease, they gave us plant remedies but if it is very bad … we will have to go to the hospital or inject you with an antidote.
Special attention should be given to this limitation regarding progression, symptoms and treatment of CD. Together this data also identified limited knowledge about CD transmission as a barrier to the implementation of health promotions.
Stigmatization of the disease: Participants were ashamed to admit that they had seen a chinchorro, especially if it had been present inside the house. Some participants, for instance, mentioned that they had never seen a bug before. However, as the interview advanced, they admitted they had killed one. Additionally, they often saw the presence of the bug as a sign of a lack of hygiene and poverty. For instance, a 14-year-old said:
… people with low incomes that still live in mud houses of adobe … some places don’t even have water or electricity. They live like that. They accumulate things, materials, garbage … That’s where I think you mostly find the bug.
This repeated use of ‘them’ and ‘they’ separated people at risk of home infestation as an ‘other’ divided from the regular portion of the community. Participants directly connected poverty and economic status to the presence of the triatomine bug. Moreover, this connection may stigmatize the disease or exposure to its risk factors. A higher risk of having the disease was also associated with age, as older people and children were seen as more at risk. The youth, however, did not consider themselves at risk. Together these misconceptions represent a limitation for the implementation of prevention practices; they also represent a limitation to accessing health treatment. Stigmatization of the disease could also limit participation in surveillance. Thus, it is critical to acknowledge stigmatization among the studied population.
Youth as agents of change
The second category was exploring ways in which youth can become agents of change. Within this category, two themes were identified. First, youth were interested in being agents of change, both by learning more about CD and by adopting practices to limit infestation. Second, they recalled play-based strategies as meaningful strategies that prompted them to desire change. The first theme indicates a willingness of youth to become involved; the second suggests the best way to encourage this involvement.
Youth are interested in becoming agents of change: Overall, participants were willing to learn about CD. Participants also expressed their interest in sharing information with other members of the community. For instance, participants mentioned their eagerness to transfer such information to other members, especially to ‘the most vulnerable members like children’. Special interest in projects where they can ‘feel empowered’ was constantly mentioned. For instance, an 18-year-old from Bellamaria mentioned, ‘last year we participated … we did a video clip, about the student life, how is it living here and coming from the city, I liked that’. This kind of interest from youth in learning about CD as well as being part of prevention projects represents an opportunity for intervention. More importantly, the inclusion of this targeted population could not only incentivize youth but also empower them.
Identifying best strategies: Participants mentioned the importance of cleaning the house and surroundings, chicken nests, and avoiding the accumulation of materials such as wood or brick. A 15-year-old youth mentioned his active participation in prevention practices:
… changing the chicken nest often, avoiding the accumulation of wood, bricks around the house. We have to cover the holes, clean the house in depth and clean the beds and the mattress.
When participants were asked about where they had learned prevention practices, they mentioned that the knowledge came from their parents and grandparents or external agents. An 18-year-old female from Bellamaria said:
… we were taught by people from the university, when they came the first time, they teach us little by little and we were learning … we should not allow animals inside the house and that we should keep our bed tidy, otherwise the little animal, the ‘chinchorro’ could come and bite us.
Participants were also invited to discuss previous intervention programs and the impact they had had on their lives. Vivid memories were present regarding the chinchorro and association with the disease. Overall, games organized by external agents during their visit were the most memorable for the participants. For instance, a participant from Bellamaria said:
… they gave us activities on how to prevent the bite of the ‘chinchorro’ … they taught us that we have to have our house clean and holes on the walls had to be covered.
… we used to play a game with a ball … and the one that has the ball and put it on the arch … and there the new ones become the ‘chinchorro’ … they covered your eyes … you have to put a ball ‘chinchorro’ in the hand and if you won, they gave you a prize.
Overall, ludic activities for learning about CD prevention practices were impactful. More importantly, participant recollection of learning games was constantly mentioned, especially the played-based strategies, which not only bring good memories to participants, but they also remain over time17-19. Future intervention programs should adopt this type of play-based strategies in youth populations. Together these results highlight some of the positive impacts of intervention programs and the importance of entertainment education to promote community-based disease prevention.
The authors also found some limitations among participants such as lack of knowledge about CD transmission, symptoms, and treatment or stigmatization of the disease. Perhaps future entertainment education programs should emphasize the importance of learning about CD transmission.
Discussion
This study aimed to understand the knowledge regarding some aspects of Chagas disease and how intervention programs for the youth population living in the southern region of Ecuador are remembered. The aim of the first research question was to assess the current state of CD knowledge among youth in rural communities of southern Ecuador. Results showed that there is cursory knowledge about the triatomine, prevention practices and vector transmission, yet there is a disconnection with CD and its transmission. Additionally, the authors found that there were substantive gaps in knowledge about CD symptoms and treatment. Although participants seem to recognize the kissing bug or how to prevent colonization in their homes, they did not know that the kissing bug can transmit CD. Furthermore, participants did not have a clear concept of what CD is and the consequences of living with it. The study results identified this as an important gap when implementing intervention programs, which could contribute to an underestimation of communities’ risk of CD.
The authors also identified a lack of proper implementation of prevention practices among participants. Participants’ improper handling of the bug if encountered inside the house, maintenance of domestic animals inside the house, and failure to report the presence of the bug to the authorities further reflect a lack of association of triatomine bugs with disease risks. These behaviors have been associated by other authors with a lack of knowledge about Chagas disease and its transmission28. In agreement with other authors, the present study’s results showed that greater knowledge of CD could have the potential to drive communities to enact new preventive health-related behaviors29,30.
Youth from the communities also articulated a stigma associated with the presence of the bugs inside the house. Overall, participants were ashamed to confirm the presence of the bug inside their houses. They associated the kissing bug with lower socioeconomic status. These associations may limit the implementation of prevention practices because people are ashamed to ask for help, for fear of being stigmatized in their communities31. Stigmatization of CD has become a major psychological barrier for accessing health treatment for this disease32. In addition, previous studies have found that the public associates CD with filth, neglect and misery, leading at-risk populations to ignore possible infections28. It may also be a psychological barrier to primary prevention practices. Future education programs should be encouraged to address and counter stigma in CD prevention.
Previous research has found that effectively disseminating information about the vector and the disease to the population at risk has helped prevention programs to be more effective11. Therefore, education campaigns linking the vector with the disease and parasite may be a promising strategy to adopt in rural southern Ecuador.
The aim of the second research question was to identify which components of an intervention program youth identify as motivating to participate in control programs. Results showed that youth participants identified external agents as an important source of information that could motivate prevention and control efforts toward CD. Participants stressed the importance of programs for children and how they would like these interventions to be performed for future generations. Additionally, participants repeatedly commented on how prevention practices were encouraged and taught by parents, grandparents and external agents. The generational transfer of information appears to play an essential role in replicating behaviors, but improved behaviors can also result from the efforts of external agents that engage youth in the communities.
This study confirms the importance of children and youth being involved in educational vector control programs19. More importantly, information is retained and transferred over the years. Youth can play an essential role in intervention programs because household activities can shape actions throughout adult life30. The present results confirm findings from work with youth in Mompós, Colombia33 and Córdoba, Argentina34 that young people are willing to participate in surveillance and control programs for CD, as well as their findings that there are significant shortcomings in understandings of CD vectors and etiology that should be addressed to make this surveillance and control most effective. Thus, active participation and empowerment of youth populations may be a promising approach when developing effective CD control programs in the Andean Ecuador region.
Conclusion
Overall, the authors conclude that intervention programs like that of the HLI have had a positive effect on youth in the communities by delivering information regarding the parasite vector and supporting general prevention practices. Nevertheless, several limitations and gaps of the HLI intervention program were identified. For instance, the study found that there is still a disconnect between the risk of having the kissing bug living inside houses and knowledge about CD transmission. Thus, these results support findings that community members underestimate their risk of CD10. This lack of knowledge regarding Chagas disease should be considered as a significant barrier for successful vector control programs. Even though knowledge is not enough to change behaviors29, addressing these gaps could be a starting point for improving intervention programs. Understanding CD and the social context that influences people’s living conditions is an important factor in explaining the prevalence of the disease and increasing public awareness of it28. Gathering further information from other members of the communities can confirm or deny these claims about general community knowledge surrounding CD.
Finally, the authors addressed the importance of improving and revisiting intervention programs such as that of the HLI when working with youth in the communities. Messages should focus not only on preventing disease transmission or evoking fear of the kissing bug, but on preventing further stigmatization of the disease in the communities. Acknowledging barriers such as misinformation, and limited knowledge about transmission or stigmatization of the disease, could help design better campaigns for prevention behaviors that tailored to the targeted communities.
Limitations of the study
Limitations during the development of this study were identified. The researchers in this study are affiliated with the HLI, providing them with insight and access to the processes and outcomes of these efforts. At the same time, knowledge of participants who had been previously involved with HLI may have led some participants to provide overly positive responses regarding HLI’s efforts. Because of the logistical organization of the study, some participants might have discussed their answers beforehand on the topics of the interview. However, the compressed 2-day timeframe made this sharing unlikely. Finally, this study only included youth who had been involved in previous education programs. Thus, these findings should not be generalized to all youth or other members in the communities but instead considered as potentially transferable lessons.
References
You might also be interested in:
2011 - Nature and nurture in the family physician's choice of practice location