

Dear Editor
I would like to draw your readers' attention to the plight of the Sahariya tribe who live in various districts of Madhya Pradesh, central India. Sahariya means 'inhabitants of the jungle' (from the Persian word Sehr), and most of the year these people live in small villages called 'sahrana', dependent on the forest for produce and shelter (Figs1,2). However, for approximately 3 months of the year the tribe travels in search of work. At this time they are vulnerable to infections and other health hazards. As a result, tuberculosis (TB) is prevalent in this tribe.

Figure 1: Sahariya tribespeople.

Figure 2: A typical Sahariya house.
The present pilot study was conducted in the year 2005-2006 as an initial screening for TB prevalence in the three most populated tribal villages (Kalmi, Kakerdha and Daingda, MP). A researcher and staff of the Revised National Tuberculosis Control Program (RNTCP) conducted a village-to-village survey and collected sputum and blood samples from 355 randomly selected individuals, after obtaining informed consent. Sputum smears were prepared and subsequently participants were divided into groups: sputum three positive, two positive, one positive and sputum negative, as per standard RNTCP protocol1. Sputum-positive participants were investigated by chest X-ray.
The study revealed 46% samples (n = 164) to be positive for acid fast bacilli (AFB; Fig 3); 53.8% was negative (n = 191). Of the AFB-positive cases, 42.8% and 31.7% were taking TB chemotherapy categories I and II, respectively.
Serum levels of certain pathologically important isozymes, such as LDH, were estimated (Fig 4; serum LDH level has been reported to be elevated in the presence of tissue injury and damage2). In sputum-positive cases, the total serum LDH was found to be significantly elevated (p<0.0001), with mean values of 304.31 ± 252.1 IU in sputum two-positive individuals, and 365.63 ± 262 IU in sputum three-positive individuals, compared with the sputum-negative sample of 232 ± 155.91 IU. There was no association of disease with sex.
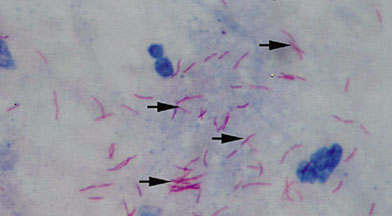
Figure 3: Sputum three-positive slide showing AFB.
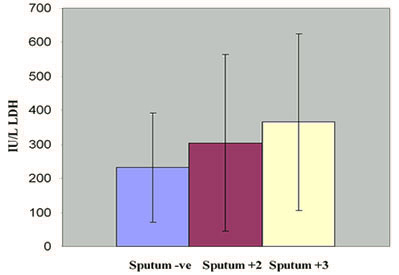
Figure 4: Serum LDH levels for negative and positive sputum samples.
None of the other tribal groups in the state have been reported to have such a high prevalence of tuberculosis. Our attention was drawn to this from the unusually high number of Sahariya TB patients reported by the district hospital, and a published report3 which compared the Sahariya disease prevalence with a neighboring tribal community. The situation of the Sahariya tribe is alarming and requires serious medical attention, and further extensive research on the possible role of environment, ethnicity and genetics in their increased susceptibility to TB.
Prithvi R Sharma
Pramod K Tiwari
Department of Molecular & Human Genetics
School of Studies in Zoology, Jiwaji University
Gwalior, MP, India
References
1. Ministry of Health & Family Welfare. RNTCP at a glance. New Delhi: Central TB Division, Directorate General of Health Services, Ministry of Health & Family Welfare: India, 2006.
2. Lossos IS, Breuer R, Intrator O, Sonenblick, M. Differential diagnosis of pleural effusion by Lactate Dehydrogenase isoenzyme analysis. Chest 1997; 111: 648-651.
3. Chakma T, Rao PV, Pall S, Kaushal LS, Dutta M, Tiwary RS. Survey of pulmonary tuberculosis in a primitive tribe of Madhya Pradesh. Indian Journal of Tuberculosis 1996; 43: 85.