
Introduction
Adolescence is generally considered a healthy period of life1. However, adverse sexual and reproductive health (SRH) outcomes threaten the physical health and psychological wellbeing of adolescents, particularly those in low- and middle-income countries (LMICs)2. The adolescent period is characterised by significant cognitive, emotional and physical change3; it embodies the critical transition between childhood and adulthood. During this life stage, young people develop their own sexuality, become aware of gender roles and gain an increasing interest in sex and intimate relationships2. Many adolescents do not develop the impulse control or rational decision-making capacity to safely navigate through this period, particularly during their early sexual experiences, leaving them vulnerable to adverse SRH outcomes2.
Adolescent SRH is of particular concern in Cambodia due to the country’s large and rapidly growing adolescent population4. The 2014 Cambodian Demographic Health Survey reported that 43% of the Cambodian population are aged less than 19 years4. Today’s Cambodian youth are the children and grandchildren of the Khmer Rouge survivors. They have grown up in a politically and socially different landscape to their parents. They experience higher levels of educational attainment, more freedom and increased access to the global community through advances in technology, communication, travel and commerce. The increased social and economic freedoms experienced by the current generation of adolescents, particularly those relating to population mobility, have forced Cambodian youth to navigate SRH challenges not encountered by prior generations, arguably leaving them more vulnerable to adverse SRH outcomes.
Adolescent SRH is particularly important amongst indigenous populations in the north-eastern provinces of Mondul Kiri and Ratanak Kiri. Marginalised by physical remoteness, poverty and cultural barriers, adolescents in these provinces experience comparably worse SRH outcomes than the national averages (Table 1); of particular concern is the prevalence of adolescent pregnancy. Thirty-four percent of girls aged 15–19 years in Mondul Kiri and Ratanak Kiri provinces have begun childbearing; this is almost three times higher than Cambodia’s national average of 12%4.
The prevalence of adolescent pregnancy amongst indigenous populations in north-eastern Cambodia is concerning given the adverse health, social and economic implications of early childbearing. The United Nations Population Fund (UNFPA) reports that tens of thousands of adolescent girls die each year due to pregnancy- and childbirth-related complications5; such complications are identified as the leading cause of death for girls aged 15–19 years worldwide6. The children of adolescent mothers are also at increased risk of experiencing adverse health outcomes, with an increased prevalence of low birth weight, preterm delivery and severe neonatal conditions amongst the children born to adolescent mothers7. Additionally, adolescent pregnancy often results in young girls leaving school early, which reduces their ability to contribute financially to their households and contributes to the intergenerational transmission of poverty8.
Ratanak Kiri Province is located in the north-east of Cambodia, bordering Lao to the north and Vietnam to the east9, and has a population of approximately 200 00010. There are eight indigenous population groups in Ratanak Kiri Province and they make up more than 75% of the total population11, with the Tompoun and Jarai identified as the most common indigenous population groups12. Collective decision-making is a core value of indigenous populations in Ratanak Kiri Province and villages are organised to promote social cohesion12. Villages are often centred around a large communal meeting place where community members come together for meetings and cultural ceremonies. The relative autonomy of indigenous groups in the province requires strong leadership from village chiefs and other respected village elders12. Village elders have significant decision-making power and a strong educational role in terms of sharing traditions and beliefs with younger generations.
Language, cultural and geographic barriers have restricted qualitative exploration of the unique SRH challenges that face indigenous populations in Ratanak Kiri Province. This study sought to explore adolescent mothers’ perceptions and knowledge of their reproductive bodies and to identify sources from which adolescent mothers receive information about SRH as a means of understanding the SRH challenges that face this population group.
Table 1: Sexual and reproductive health and related behaviours in Ratanak Kiri/Mondul Kiri provinces and national averages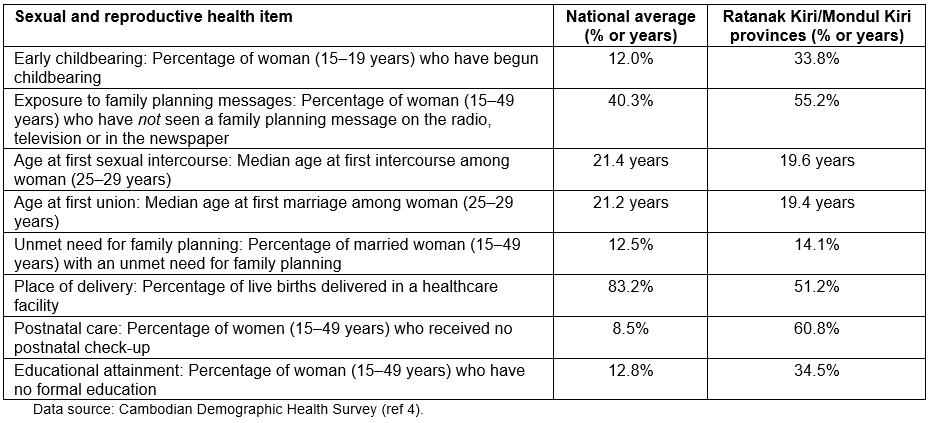
Methods
Theoretical framework
The socioecological model (SEM) was used as the analytical lens to explore the SRH challenges that face adolescent mothers in Ratanak Kiri Province. The SEM was first introduced by Bronfenbrenner13 and has been adapted to a wide variety of topics and settings since this time. The SEM provides an understanding of the many levels of a social system and the interactions between individuals and the environment within this system14. There are several versions of the SEM, which adopt slightly different classification systems. The four-level SEM employed by the Centers for Disease Control and Prevention was adopted for this study15. The first level (individual) considers individual biology and personal characteristics such as age and income, the second level (relationship) considers an individual’s social networks including their family and close friends, the third level (community) explores the settings in which individuals spend the majority of their time, including education settings and workplaces, and the fourth level (society) includes the broad societal factors that impact upon health including health, economic, educational and social policies16.
The multilevel SEM was considered most appropriate for this study because of the complexities associated with the SRH of adolescent mothers in Ratanak Kiri Province. Individual behaviour change is required to reduce adolescent pregnancy rates and improve SRH outcomes; however, individual behaviour change is influenced by factors at different levels. For example, SRH knowledge at an individual level may be influenced by factors at a relationship level (eg social networks and cultural expectations), community level (eg geographic accessibility to educational and health services) and society level (eg national SRH policies). Understanding how factors on each of these levels contribute to the poor SRH outcomes experienced by indigenous adolescents in Ratanak Kiri Province will aid in the development of appropriate strategies and programs that encompass these key factors.
Research design
A qualitative descriptive approach was employed to explore the SRH knowledge of adolescent mothers from indigenous populations in Ratanak Kiri Province. All participants engaged in a combined body mapping exercise and semi-structured interview. The qualitative approach allowed the researcher to go beyond the quantitative data published in the 2014 Cambodian Demographic Health Survey to explore the SRH challenges experienced by indigenous adolescents in Ratanak Kiri Province, with a particular focus on their level of SRH knowledge and sources of SRH information.
Fieldwork
The fieldwork was conducted by the first author, a bilingual research assistant (third author) and two local translators in January and February 2017. The research assistant, who has a Master of Public Health, is a Cambodian national who is fluent in Khmer and English languages and has conducted similar qualitative studies that have employed body mapping exercises and semi-structured interviews to explore SRH issues among Cambodian women. The two local translators (Jarai and Tompoun) were provided by a local non-government organisation (NGO) working in the healthcare sector in Ratanak Kiri Province. The local translators helped with translation in instances where the participants required additional assistance with comprehension or communication. The inclusion of local translators helped to reduce language and cultural barriers that have previously restricted or prevented research among this population group. A two-day training workshop was held with the research team to pilot test the interview guide and to ensure that the research team members understood the purpose of the study and were clear on their role.
Participant recruitment
Participants were purposively sampled from seven villages in Ratanak Kiri Province (Table 2). To be eligible for recruitment, female participants were required to be from the Jarai or Tompoun indigenous group, aged 15–19 years and have had at least one live birth. Seven villages were randomly selected from a list of Tompoun and Jarai villages in Ratanak Kiri Province provided by the local NGO. Meetings were scheduled between the research team and the seven village chiefs to explain the purpose of the study and request permission to conduct participant recruitment and data collection in the village. The seven village chiefs agreed to assist the research team and provided the names and ages of adolescent mothers in their village. The research team attempted to visit each of the adolescent mothers identified by village chiefs to confirm their eligibility and explain the purpose of the study. If adolescent mothers met the selection criteria and agreed to participate, a time and date were scheduled for data collection. Only one mother approached by the research team declined to participate in the study.
Table 2: Distances from health facilities of study villages and indigenous groups 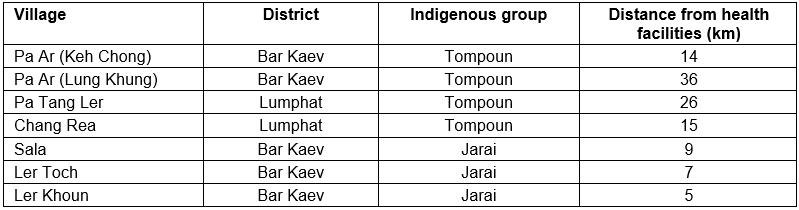
Participants’ demographic characteristics
The study sample consisted of 22 adolescent mothers, aged 15–19 years, from seven villages in Ratanak Kiri Province. The demographic characteristics of the sample are detailed in Table 3.
Table 3: Study participants’ demographic characteristics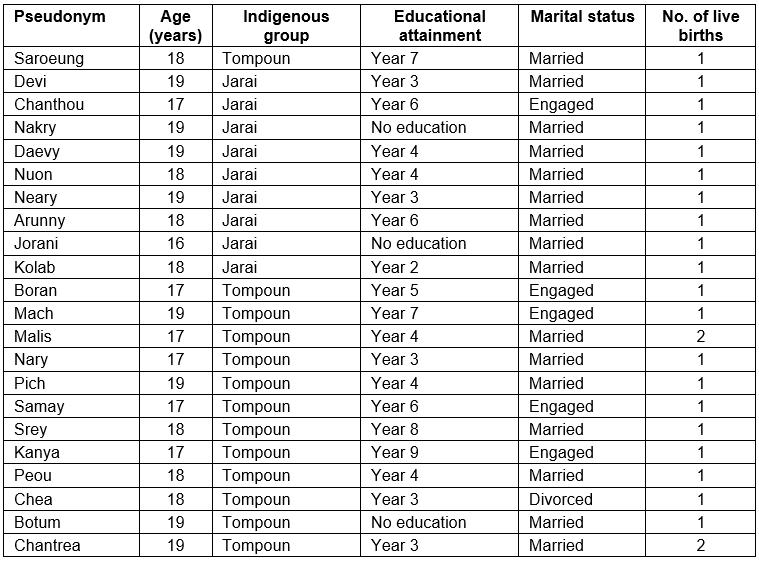
Data collection
Body mapping exercise: Body mapping exercises were used to determine participants’ knowledge of their own reproductive bodies. The researcher mapped the outline of a female body onto a large piece of paper and asked participants to use a marker pen to draw a female’s internal organs on the body map to determine their understanding of the anatomy of the human body. Participants were then given a marker of a different colour and asked to draw the female reproductive organs on the body map (Fig1). Participants were asked to explain their drawings to evoke conversation and to explore their knowledge about their reproductive bodies.
A second drawing exercise was employed to determine participants’ understanding of the menstrual cycle (Fig2). A large circle was drawn to depict the length of participants’ menstrual cycle. Participants were then asked to state the average duration of menstruation, which they coloured in red on the diagram. The researchers used the diagram as a focal point to ask participants questions about their menstrual cycle and fertility. For example, participants were asked, ‘Can a woman get pregnant while she is bleeding?’ and ‘What is the most fertile part of the menstrual cycle?’
Body mapping was identified as the best qualitative data collection method to use in this context because it reduced language and cultural barriers and was a means of engaging young participants in conversations about SRH issues. The body mapping method has been used in SRH studies globally as it has the potential to transcend national and cultural boundaries17. Cornwall employed the body mapping method in rural Zimbabwe to explore participants' understanding of the anatomy and physiology of the female body18. Cornwall suggests that the body mapping exercise provides a suitable alternative for women who may find it difficult to verbalise their knowledge of the female reproductive body, by allowing participants to give a visual account of their level of knowledge18. Additionally, the body mapping exercise aids in reducing bias that may arise from the use of Western anatomical terminology when asking direct questions about the female reproductive body18.
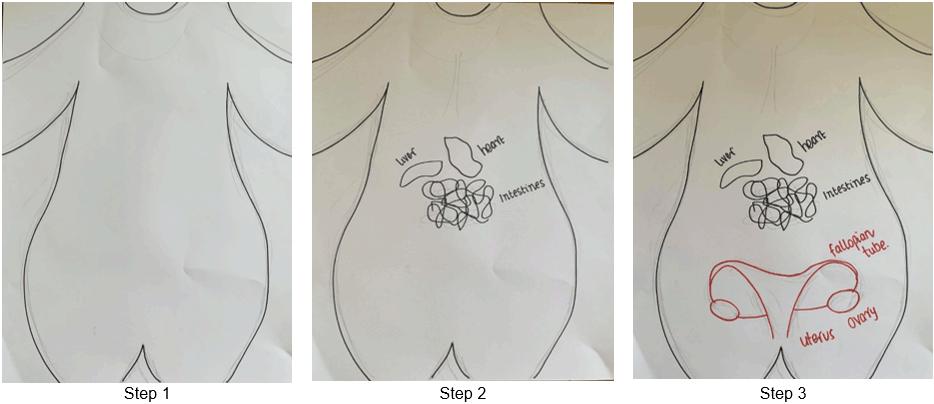 Figure 1: Example of steps taken during the body mapping exercise.
Figure 1: Example of steps taken during the body mapping exercise.
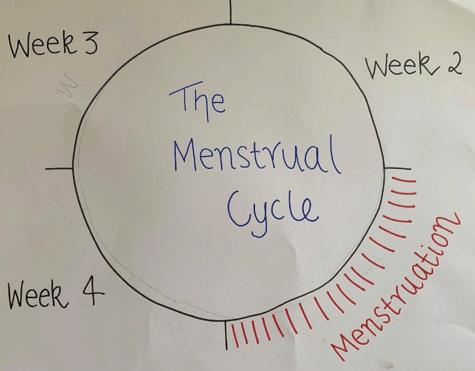 Figure 2: Example of the menstrual cycle drawing activity.
Figure 2: Example of the menstrual cycle drawing activity.
Semi-structured interview: A semi-structured interview was conducted to further explore participants’ SRH knowledge and determine the key sources of this knowledge. An interview guide with a set of open-ended questions was developed prior to the commencement of the study and pilot tested before use. However, there was flexibility for the researcher to expand on these questions through the use of probes and to ask additional questions. An interview guide ensured the topics covered in the interview addressed the study objectives and were consistently asked to all participants. Once interviews had been translated from Khmer and transcribed into English, member checking was employed with all participants to ensure the accuracy of the data19 and to increase rigor20. Data saturation was reached after semi-structured interviews were conducted with 22 adolescent mothers.
Data analysis
Digital recordings were translated into English by a trained bilingual social researcher who was unfamiliar with the topic and study design. Thematic analysis was used to analyse the semi-structured interview transcripts. Body maps were visually examined in conjunction with analysis of the transcripts. The data analysis processes were adapted from the step-by-step guide to thematic analysis offered by Braun and Clarke21. Table 4 details the data analysis process. Thematic analysis was performed by the first author and included regular communications with authors to discuss the analysis process and emerging themes.
Table 4: Data analysis process 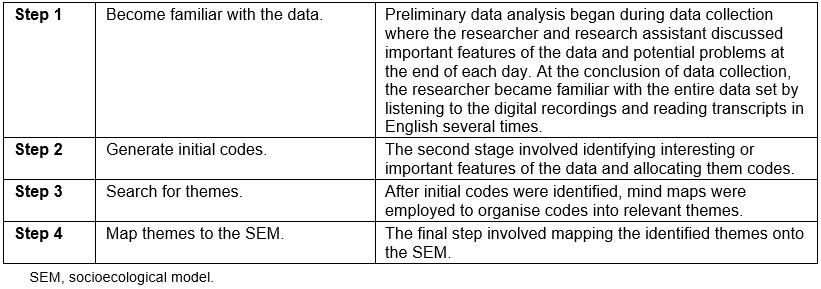
Ethics approval
The study was approved by the Deakin University Human Research Ethics Committee (2014-159) and the Cambodian Ministry of Health Human Research Ethics Committee (027NECHR). A plain language statement, detailing the purpose of the study, was verbally delivered to participants in the language they felt most comfortable with (Khmer or indigenous language) and then informed consent was obtained from all participants.
Results
Sexual and reproductive health knowledge
Participants demonstrated limited SRH knowledge, including that pertaining to the anatomy of the female reproductive body, the physiology of human reproduction, fertility and pregnancy.
Anatomy of the female reproductive body
Adolescent mothers demonstrated a partial understanding of the anatomy of their reproductive bodies (Fig1). Seventeen adolescents were able to verbally identify the uterus as an organ of the female reproductive system. However, they had difficulty drawing and locating the uterus on the body map. Adolescents identified other reproductive organs including the placenta and vagina. Five adolescents referred to a ‘reproductive organ’ but were unable to explain the function of this organ. No participant described the ovaries, fallopian tube or cervix on their body map.
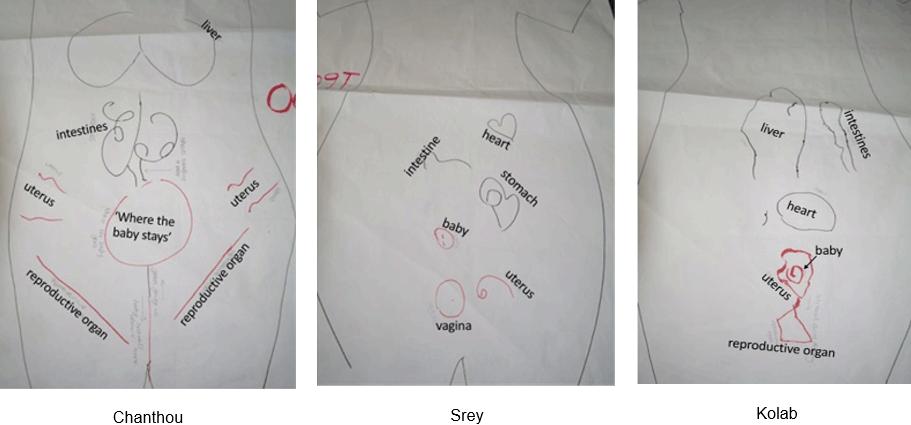 Figure 3: Images of body maps by Chanthou, Srey and Kolab.
Figure 3: Images of body maps by Chanthou, Srey and Kolab.
Physiology of human reproduction
All adolescent mothers understood that a woman becomes pregnant after engaging in sexual intercourse. Adolescents with limited SRH knowledge could not expand on this to explain the physiology of human reproduction. Those with a higher level of knowledge about the reproductive system explained that women become pregnant when a male’s ‘water’ or ‘blood’ enters the female reproductive system during sexual intercourse and mixes with a female’s ‘blood’. Few adolescents could explain the route of the sperm through the reproductive system or identify where and how fertilisation takes place.
Fertility
All adolescent mothers had some knowledge of the menstrual cycle and were able to state the approximate length of their own menstrual cycle. However, no participant could describe the physiology of the menstrual cycle and why women menstruate.
I sometimes feel dizzy, but I am unsure what causes the blood to come out. (Chanthou)
I am used to it [menstruation], but I still don’t know what causes it. (Kolab)
The relationship between the menstrual cycle and fertility was poorly understood. Six adolescent mothers believed they were not fertile during menstruation.
As there is bleeding at that time [menstruation] the baby cannot be made. (Chea)
In contrast, several adolescent mothers believed that menstruation was the most fertile phase of the menstrual cycle. Eighteen adolescents believed that they could get pregnant during the other three phases of the menstrual cycle: follicular, ovulation and luteal. No participant correctly identified the most fertile part of their menstrual cycle.
Pregnancy
Adolescent mothers understood that the average duration of pregnancy was 9 months. However, they demonstrated a limited understanding of gestation beyond this point. The majority of adolescents explained that eating ‘healthy’ or ‘nutritious’ foods during pregnancy would enable the baby to develop.
The mother eats a lot of food, like meat, veggies and fruits, so the baby can get that food too. (Chea)
Further probing suggested that adolescent mothers who had been in contact with healthcare providers during pregnancy were advised about the types of foods they should eat. The majority of participants attended the local healthcare centre on at least one occasion during the prenatal period. Adolescents were unsure how a baby received nutrients from the mother during pregnancy; several suggested that a baby may receive nutrients from the mother through the intestines or stomach, but they were unable to explain how this process occurred. No participant understood the role of the placenta or umbilical cord in relation to the development of a foetus.
She eats the food, and it goes through the intestine, and then go to the baby … it is the intestine that delivers food to the baby. (Saroeung)
When the mother eats and the food goes into the stomach, the baby would receive it. (Kolab)
Adolescent mothers were encouraged to use their body map to explain the physiology of childbirth. Kanya understood that during childbirth a baby ‘is born through the vagina’. However, Kanya was unsure of the birthing process and the role of the uterus during pregnancy and childbirth. This was a common gap in SRH knowledge among the adolescent mothers.
Factors influencing adolescents’ sexual and reproductive health knowledge
Participants limited SRH knowledge was influenced by factors on individual, relationship, community and society levels (Fig4).
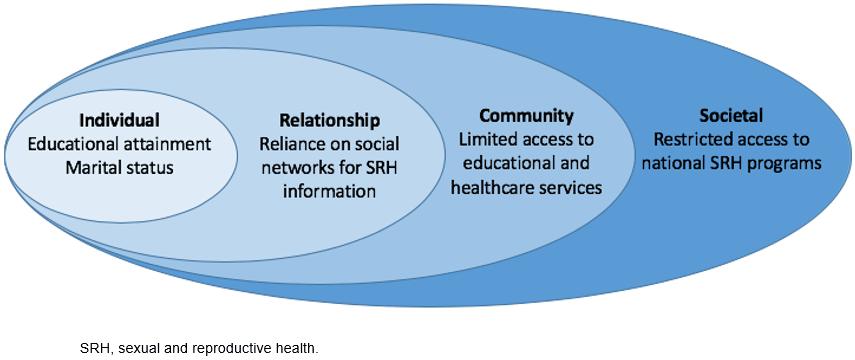 Figure 4: Key themes mapped onto the socioecological model.
Figure 4: Key themes mapped onto the socioecological model.
Individual
Low educational attainment: All adolescent mothers had ceased formal education at the time of data collection and the majority had dropped out of school prior to finishing their primary school education. Low educational attainment is not only identified as a barrier to health information; participants with lower educational attainment have fewer opportunities to develop their Khmer language skills.
Child marriage: All participants were engaged or married before the age of 18 years. Participants identified early marriage as a key barrier to completing their formal education.
I already got married. How I could stay at school? (Arunny)
Relationship
Reliance on social networks for SRH information: Adolescent mothers repeatedly stated that female family members and village elders were their primary source of SRH information. Adolescent mothers either had conversations with female family members or learnt vicariously by listening to other women in the village talk about their experiences of pregnancy and childbirth. Kolab, an 18-year-old mother from the Jarai indigenous group, explained that her mother taught her about the female reproductive system and pregnancy after she became pregnant with her first child. Prior to this conversation she had limited knowledge of pregnancy and childbirth. Kanya, a 17-year-old mother from the Tompoun indigenous group, learnt about the female reproductive system, in particular pregnancy, by ‘listening to other people's conversations, especially those [women] who have had a child’. Vicarious learning provided a source of inaccurate information and misconceptions for many adolescent mothers. Kolab’s conversation with her mother led her to believe that a baby develops in a woman’s intestines during pregnancy.
Community
Interactions with healthcare staff: Visits to the healthcare facilities, particularly during the prenatal period, provided adolescent mothers with an opportunity to access accurate SRH information. For many adolescent mothers this was the first time they had been exposed to SRH information.
I went to the hospital for an ultrasound during my pregnancy and that is how I know about it [pregnancy and childbirth]. (Botum)
I heard about it from the birth attendant … when I was having an ultrasound. (Chantrea)
Prenatal visits to the healthcare centre also provided adolescent mothers with access to information about modern contraception.
The doctors told me that if I take the pill, it will give birth spacing from 2 to 3 years. (Tevy)
There were occasions when medical professionals and health volunteers visited their villages to share SRH knowledge. The four adolescent mothers from Chang Ra, a Tompoun village in the Lumphat District, said they received SRH information from medical professionals or health volunteers in their village; this was their primary source of SRH knowledge. Chea explained that her father, who was a health volunteer, holds monthly meetings at their home to discuss contraception. All members of the village are welcome to attend these meetings, regardless of their age, gender or marital status.
Both husbands and wives [attend the meetings] so there is a mix of everyone … single people are present too. (Chea)
Adolescent mothers from Chang Ra village explained that a medical professional from the provincial hospital had visited the village and provided SRH information to pregnant women.
The doctor from the provincial hospital has been here before and had an interview. He told me what should be done and gave me some advice about pregnancy and contraception. (Peou)
Society
Restricted access to national SRH programs: The majority of adolescent mothers did not have regular access to a television, radio or a smartphone and consequently their exposure to SRH health information through these mediums was limited. Adolescents’ limited access to communication technology provides a barrier to national SRH programs that use these platforms to deliver SRH information. For those who did have access to a radio, language barriers prevented information acquisition in this way. Kolab was aware that there were reproductive health programs in the Khmer language on the radio and television but language barriers prevented her from obtaining sufficient SRH knowledge from these programs. She explained, ‘there is a program about reproductive health on TV and radio … because they speak very fast I only got some of it’.
Discussion
Adolescent mothers demonstrated a limited understanding of SRH issues including the anatomy of the female reproductive body, the physiology of human reproduction, fertility and pregnancy. This was consistent across the sample, irrespective of age, educational attainment and distance from healthcare facilities. No participant was able to accurately identify the most fertile phase of their menstrual cycle; this has significant implications for adolescent girls who want to effectively assess their risk of getting pregnant22.
Rajapaksa-Hewageegana and colleagues found 17% of pregnant adolescents in Sri Lanka could correctly identify the most fertile part of their menstrual cycle23. Similarly, an evaluation of the Demographic and Health Survey data from 18 sub-Saharan African nations found that 18% of adolescents aged 15–19 years were able to correctly identify the time of ovulation24. These findings suggest that adolescent populations in low- to middle-income countries do not have a comprehensive understanding of fertility. However, results from the present study suggest that a lack of fertility knowledge is particularly problematic amongst indigenous populations in Ratanak Kiri Province.
Adolescent mothers’ limited SRH knowledge may be explained by the lack of accurate information available to indigenous populations in Ratanak Kiri Province. The primary source of information about the menstrual cycle and fertility was adolescents’ mothers and female village elders. This finding is consistent with research from Ghana25, India26 and Jordan27 that cites mothers and female relatives as the primary source of SRH information for adolescent populations. This is problematic for several reasons. First, discussing SRH issues is taboo in the Cambodian culture28 and therefore Cambodian woman may feel embarrassed sharing important SRH information with unmarried adolescent females. This finding is consistent with previous research that identified cultural taboos surrounding conversations about menstruation as a barrier preventing parents from discussing SRH issues with their adolescent children29. Second, female relatives and friends may not be adequately informed about SRH issues to enable them to deliver this information to adolescents. The adolescents’ mothers, grandmothers and village elders have received limited education about SRH issues themselves and are therefore unable to educate the young women about SRH.
Adolescents in Ratanak Kiri Province have limited access to accurate sources of SRH information, which may explain their reliance on the incorrect information they receive from their mothers and female villagers. Adolescents living in rural and remote areas of Cambodia are yet to benefit from the technological advances that have provided their urban counterparts with additional sources of SRH information. The UNFPA and United States Agency for International Development funded a youth-led SRH program (Love 9) for adolescents and youth aged 15– 24 years on radio, television and the internet between 2013 and 201630. However, the majority of adolescent mothers did not have access to a radio or television and no adolescent interviewed knew what the internet was. Consequently, indigenous adolescents in Ratanak Kiri Province are unlikely to benefit from Love 9 or similar programs that utilise communication technology.
In contrast, adolescent mothers’ interaction with staff in government healthcare facilities provided them with an avenue to acquire accurate SRH information. However, adolescent mothers obtained this knowledge for the first time when they were pregnant and attended the healthcare facilities for prenatal care. Consequently participants had limited SRH information at the time of sexual initiation, when they are most vulnerable to adverse SRH outcomes.
The findings support the need for the Ministry of Education, Youth and Sport’s Comprehensive Sexuality Education (CSE) program, which was introduced into the primary and secondary school curriculum at the beginning of the 2018–2019 academic year31. Introducing SRH education into both the primary and secondary school curriculum ensures young people have access to accurate SRH information before reaching adolescents, when they become vulnerable to adverse SRH outcomes. The WHO has identified school-based SRH education as one of the most significant ways to improve adolescents’ SRH32. Education settings have the infrastructure, tools and trained staff to adequately deliver SRH programs, making it a cost-effective way to increase positive SRH outcomes32. An analysis of school-based SRH programs across six countries (Nigeria, Kenya, Indonesia, India, Estonia and the Netherlands) found school-based SRH programs were a cost effective and cost saving tool to reduce adverse SRH outcomes including adolescent pregnancy33. However, school-based programs fail to educate adolescents and young people who are not enrolled in formal education or who leave school early. Thirty-five percent of women aged 15–49 years in Ratanak Kiri Province receive no formal education, more than eight times that in Cambodia’s capital of Phnom Penh, where 4.1% of women receive no formal education4. Throughout Cambodia, the school curriculum is delivered in Khmer, rather than the indigenous dialect in the north-eastern provinces, providing an additional challenge for young indigenous populations. Consequently, many young girls from indigenous populations in Ratanak Kiri Province, particularly those who leave school early or who are not fluent in Khmer, may not experience the benefits of the CSE.
Limitations
Despite the significant findings noted, there are potential limitations of the study. The study was conducted across multiple languages, which presented linguistic challenges to the research team. Meaning can be lost when information is translated across several languages during qualitative data collection34. However, measures were taken to reduce potential communication barriers and increase rigor, including (1) the recruitment of a senior research assistant who holds a postgraduate degree in public health, is bilingual and has prior experience conducting body mapping exercises and semi-structured interviews with Cambodian women; (2) the recruitment of two indigenous translators, who spoke Khmer and the indigenous dialects and were used when adolescent mothers had difficulty with comprehension or communication in the Khmer language; (3) transcription and translation of digitally recorded interviews by an independent, bilingual research assistant; (4) daily debrief sessions between the primary researcher and the research assistant to discuss the emerging themes, which helped the research team identify inconsistencies in the data that may have arisen due to language or communication barriers.
Implications and recommendations
The study makes a unique contribution to the academic literature by exploring indigenous adolescents’ understanding of SRH issues and identifying the key sources of SRH information. In doing so the authors provide evidence to policy makers and public health practitioners about the unique needs of indigenous populations in north-eastern Cambodia. Prior to this study, there was limited qualitative information available regarding indigenous adolescents’ SRH knowledge and the challenges they face accessing accurate health information.
Limited SRH knowledge, characterised by misconceptions and inaccuracies, is central to the poor SRH outcomes experienced by indigenous adolescents in Ratanak Kiri Province. The findings provide evidence that indigenous adolescent mothers in Ratanak Kiri Province do not have an avenue to acquire accurate SRH information prior to sexual initiation. Policy makers and public health practitioners must take immediate action to provide indigenous populations in rural and remote Cambodia with access to accurate SRH information. This is paramount to not only improving SRH and economic outcomes but also to the upholding of Cambodia’s international human rights obligations. Cambodia has ratified the International Covenant on Economic, Social and Cultural Rights and the Convention on the Elimination of All Forms of Discrimination against Women and in doing so the Royal Government of Cambodia has an obligation to ensure that adolescents have the right to control all aspects of health, in particular their own fertility35. Addressing adolescent SRH is also essential if Cambodia is to meet targets outlined in the UN Sustainable Development Goals (ie to ensure universal access to sexual and reproductive healthcare services, including for family planning, information and education and to reduce maternal and neonatal mortality rates).
1. Increase school attendance
Cambodia has domestic and international human rights obligations to ensure that all Cambodians have access to formal education, regardless of their social and economic situation. The Constitution of the Kingdom of Cambodia includes the right to equal education, stating that all citizens (1) have the right to free primary and secondary education and (2) should receive at least 9 years of formal schooling36. Currently, many indigenous girls in Ratanak Kiri Province are unable to exercise their right to education. It is paramount that measures are taken to increase school attendance amongst indigenous populations in Ratanak Kiri Province to ensure health inequalities are not exacerbated.
2. Educate village chiefs to deliver non-formal, community-based education programs
Until universal access to education can be achieved, other modes of delivering SRH information to children and adolescents outside the formal education system must be utilised. This study found that adolescents’ social interaction with family members and female villagers was the primary source of SRH information. It is essential that public health action utilises this platform to increase SRH knowledge. Educating village elders and respected community members to lead community-based informal education programs would contribute to increasing SRH knowledge and reducing misconceptions and inaccuracies prevalent in villages. Listening and dialogue groups (LDGs) have been trialled as a means of delivering health information to rural communities in Cambodia37 and are proposed as an appropriate structure for community-based education. LDGs involve gathering community members to listen to and discuss live radio broadcasts37. LDGs have been found to be an effective strategy to communicate health information to women and men of reproductive age in Ratanak Kiri; evidence suggests that acquiring health knowledge through LDGs has translated into the desired behaviour change37. Conducting LDGs in the indigenous dialect has been effectively trialled in the Lumphat and Borkeo districts of Ratanak Kiri Province37 and it addresses the language barriers that may restrict or prevent knowledge translation by other means, and ensures that accurate information is delivered in a culturally appropriate manner. This health promotion initiative has the potential to empower communities by giving them greater ownership and control over their decision-making while ensuring the sustainability of the program.
3. Reduce child marriage
All adolescent mothers were engaged or married before the age of 18 years. The UNFPA defines child marriage as any formal or non-formal union where one party is less than 18 years of age38. Child marriage can detrimentally impact on a girls’ physical health and mental wellbeing38. This is particularly true in Cambodia, as in many LMICs, where there is a cultural expectation that young girls will cease formal education and become pregnant soon after getting married. The majority of adolescent mothers explained the primary reason for ceasing formal education was because they became engaged or married. Delaying marriage would provide adolescents with time to physically and mentally mature before commencing childbearing and, consequently, reduce some of the complications that may arise during adolescent pregnancy; this would also ensure adolescents have an opportunity to complete their formal education and consequently improve their capacity to contribute financially to their households and wider community.
Conclusion
Adolescents from indigenous populations in Ratanak Kiri Province have limited access to accurate SRH information, which contributes to poor SRH outcomes. Public health action must focus on increasing adolescents’ access to SRH information by employing strategies that aim to increase school attendance and to support communities to deliver non-formal SRH education programs, in order to improve adolescents’ SRH outcomes.
References
You might also be interested in:
2019 - Prevalence of unmet supportive care needs among Indigenous cancer patients across Australia
2016 - Health concerns associated with unconventional gas mining in rural Australia