





Introduction
The delivery of medical care is in continuum with diagnosing, investigating and the treatment of disease1. Information technology in medical services is used to design, build and support the delivery of health care at scale1. Advances in technology have brought sophisticated medical devices and interactive platforms to the fore to enhance diagnosis and care2. The past decade has seen tremendous changes, with technology aiding in the conceptual framework, product design, manufacture and delivery of patient care services in terms of accessibility and data2. Mobile phone is among the commonly used technology in the world today3. Advances in biomedical engineering and the development of newer devices in the healthcare sector have led to significant improvement in the effective diagnosis and treatment of diseases4.The dramatic increase in the availability of various advanced health-related applications and computational power of the mobile phones or tablets enables healthcare providers to access clinical information aided with decision tools3.
Ophthalmology practice in urban areas has evolved in the aspects of digitization of patient records through the use of various smart devices1. Currently, few online applications exist to improve management of patients with major eye diseases such as cataract, glaucoma, age-related macular degeneration and diabetic retinopathy5,6. Cuadros and Sim reported that in 1122 cases the EyePACS application helped to replace telephone and fax referrals to retina specialists, to screen the diabetic retinopathy patients via teleconsultations and to educate the students by digital grand rounds and research purposes6.
The need for effective eye health delivery in remote rural areas is compounded by the challenges to document clinical details and connect to specialists in urban centers. Ensuring the quality of eye care delivered to every patient who visits each rural vision center is vital. There is an immense need for eyecare services in rural areas in a developing nation such as India. This study describes the implementation of a novel technology tool to capture the demographic distribution and clinical presentation of patients in rural vision centers using the eyeSmart electronic medical record (EMR) app in a three-tier eyecare network in India.
Methods
A two-year retrospective review of all patients who presented to the rural vision centers of the eyecare network of LV Prasad Eye Institute (LVPEI) was performed from September 2016 to September 2018. All patient data were retrieved using all the information captured through an in-house developed eyeSmart EMR app. A standard consent form for electronic data privacy was completed by the patient or their parents or guardians at the time of registration.
The three-tier eyecare model of LVPEI includes 176 vision centers that provide primary care in districts and villages in the states of Andhra Pradesh, Telangana, Odisha and Karnataka. These are linked to 18 secondary eyecare centers, which are in turn linked to LVPEI tertiary centers in Hyderabad (Telangana), Visakhapatnam (Andhra Pradesh), Vijayawada (Andrea Pradesh) and Bhubaneswar (Odisha). A detailed description of the LVPEI model of patient eyecare delivery is described at the LVPEI website (http://www.lvpei.org/about-us).
A comprehensive eyecare examination was performed for all patients presenting to the rural vision centers of the LVPEI pyramid (Fig1) by the vision technician at the center. Based on the ocular diagnosis made by the vision technician, treatment (spectacle correction, primary eyecare procedures) was given to the patient. The patient was referred to the next level of care in the secondary centers of LVPEI if there was a need for an advanced examination such as dilated ocular examination, any diagnostic procedure or surgical care.
The center of excellence at the apex of the pyramid includes the arms of clinical and surgical care, education, eye banking, community health and research. The various subspecialty departments cater to a wide range of complex and challenging ocular conditions. The patient can be referred from any level of the pyramid to access higher care as needed across the pyramid (Fig1).
The medical records of all patients who presented to the rural vision centers between September 2016 and September 2018 were reviewed retrospectively using the eyeSmart EMR app. The demographic details and clinical presentations were captured on a tablet device. The project, which began in August 2010, has now completed the digitization of the 198 centers of the LVPEI network, which comprise four tertiary centers, 18 secondary centers and 176 vision centers across the states of Telangana, Andhra Pradesh, Odisha and Karnataka. It has facilitated about 4.7 million consultations since its inception. The system allows the documentation of clinical information in structured forms and images, which are stored in the database of the respective centers. All information from various centers is synced to a central database that allows the real-time analysis of the entire network. The development of the eyeSmart EMR app has enabled real-time connectivity for tele-ophthalmology services and documentation of clinical information for the same through the cloud.
The app enables the vision technician to register new patients, review the patient list and refer cases to the appropriate vision center (Fig2a). The patient registration is performed by capturing the demographics (Fig2b). The clinical examination forms consist of case history, refraction and ocular examination, which are entered by the vision technician (Fig2c). The final checkout, with ocular diagnosis, is performed after a comprehensive eye examination, and the patient referred to a higher center as required (Fig 2d). The vision technician enters the information in the app during the examination of the patient (Fig3) and can capture images from the slit lamp using the tablet (Fig4).
Figure 5 describes the process of the usage of the eyeSmart EMR App in the rural vision centers. A total of 501 771 patients were captured on the eyeSmart EMR app system in this 2-year period. The variables in the collected data include age, gender, geographic location, laterality of eye affected and ocular diagnosis. The patients for whom any of these variables were not recorded were excluded from the study. Each eye of the patients was diagnosed separately. Each ocular diagnosis was categorized into different ocular disorders such as amblyopia, cataract, cornea and anterior segment disorders, glaucoma, neuro-ophthalmology, ocular trauma, refractive error, retina, uvea and strabismus.
The prevalence of demographic details and clinical presentations were captured. No identifiable information of the patient was used for analytical purposes. The de-identified information was replicated into another database from where analytics were visualized using tools for the same in real time. eyeSmart EMR is an indigenously built electronic medical record system at the LV Prasad Eye Institute, India. This system was developed in-house by using open source tools such as PHP (Zend Technologies; http://www.php.net) for programming and MySQL (Oracle Corporation; http://www.mysql.com) for database management. The eyeSmart App was developed on the Android platform and is operational in the rural vision centers in the LVPEI network.
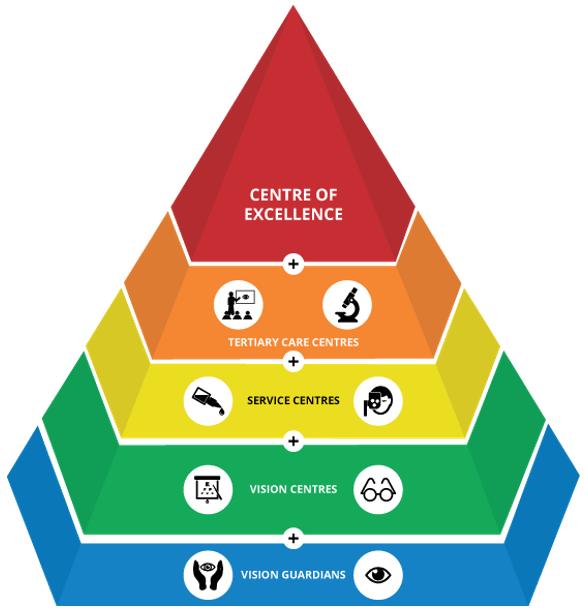 Figure 1: Pyramidal model of eye care at LV Prasad Eye Institute.
Figure 1: Pyramidal model of eye care at LV Prasad Eye Institute.
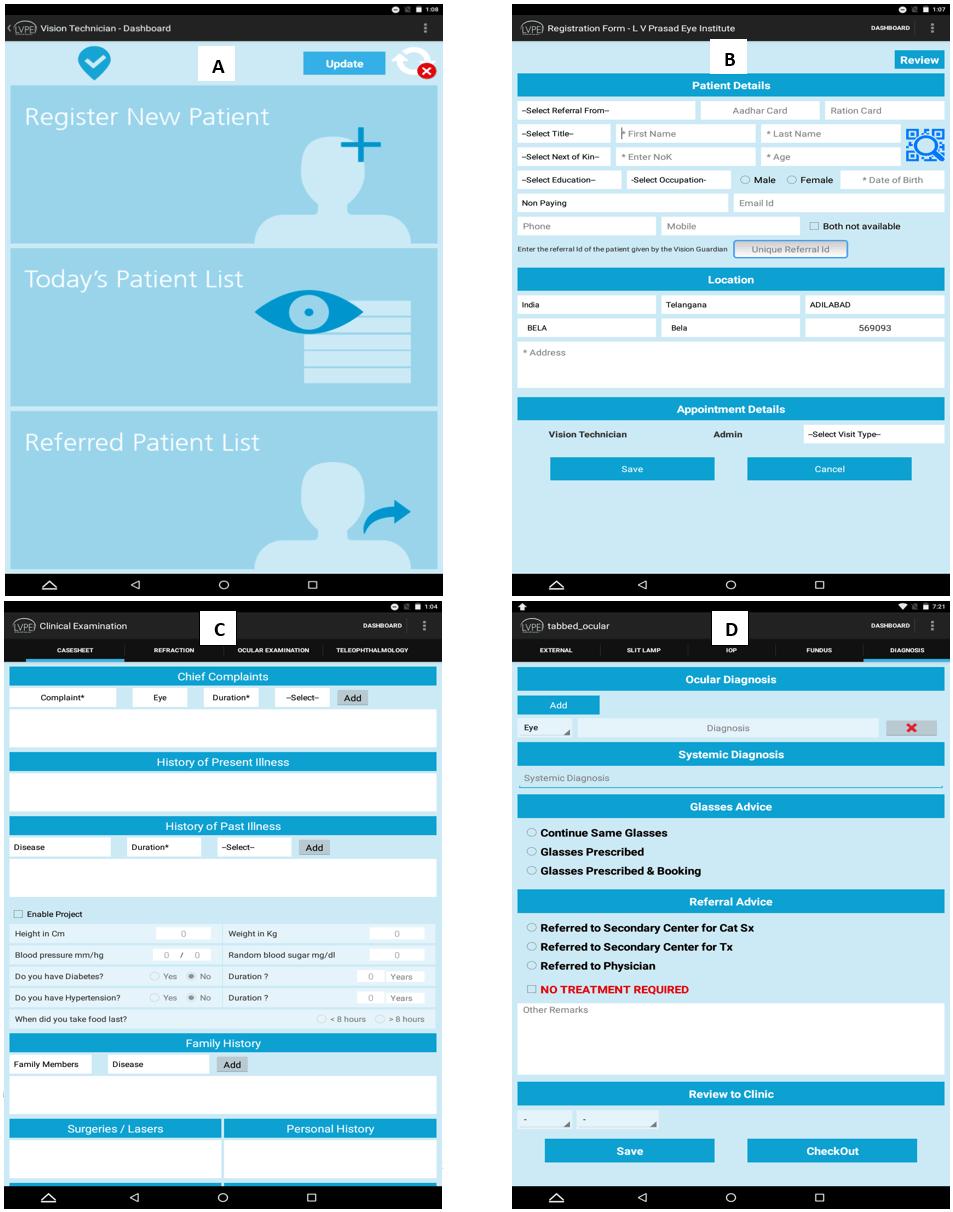 Figure 2: Dashboard of the eyeSmart electronic medical record app. B Patient registration form. C Clinical examination forms. D Checkout panel.
Figure 2: Dashboard of the eyeSmart electronic medical record app. B Patient registration form. C Clinical examination forms. D Checkout panel.
 Figure 3: Entering clinical information.
Figure 3: Entering clinical information.
 Figure 4: Capturing images from the slit lamp using the eyeSmart app on the tablet.
Figure 4: Capturing images from the slit lamp using the eyeSmart app on the tablet.
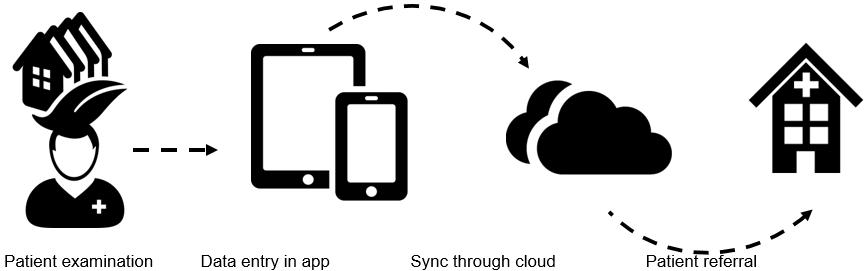 Figure 5: Process of usage of the eyeSmart EMR app in the rural vision centers.
Figure 5: Process of usage of the eyeSmart EMR app in the rural vision centers.
Ethics approval
The study was approved by LVPEI’s Institutional Review Board (LEC 07-18-117) and adhered to the tenets of the Declaration of Helsinki.
Results
Data for 501 771 patients were captured on the eyeSmart EMR app in the 2-year period. The age range of the patients was 0–100 years. The average age at presentation was 39.01 years. The number of the paediatric population (≤16 years) presenting was 62 593 (12.47%) and the number of adults (>16 years) was 439 178 (87.53%). The most common age group of the patients was 21–30 years (n=91 209, 18.18%), followed by 31–40 years (n=88 409, 17.62%). Table 1 shows the prevalence of each age category.
The ratio of males (n=273 985, 54.60%) to females (n=227 786, 45.40%) presenting to the rural vision centers was 1.2:1. A total of 617 665 ocular diagnosis instances were documented in the patients. The most prevalent ocular disorders were refractive error (n=273 720, 44.32%), followed by cornea and anterior segment disorders (n=262 974, 42.58%) and cataracts (n=67 592, 10.94%). Table 2 details the ocular disorder distribution captured through EMR. A significant proportion of ocular diagnosis was made in both eyes (n=480 782, 77.84%) followed by right eye (n=68 693, 11.12%) and left eye (n=68 190, 11.04%).
Patients presented from four states of India to the rural vision centers of the LVPEI eyecare network in the 2-year period. The most common states of presentation were Andhra Pradesh (n=337 157, 67.19%) and Telangana (n=156 482, 31.19%). Table 3 provides details of statewise distribution of patients.
Patients who required further detailed clinical examination and higher medical or surgical care were referred to the next level of care: secondary or tertiary centers of the LVPEI pyramid. The referral count of the patients from vision centers to higher centers is shown in Table 4.
It was possible to capture the prevalence of ocular disorders with the EMR system due to the standardization of the system across the network. A real-time dashboard of the demographic details of patients presenting to the rural vision centers of the LVPEI network from September 2016 on the EMR system can be accessed at http://www.lvpei.org/aeye/eyesmartapp.html
Table 1: Age distribution of patients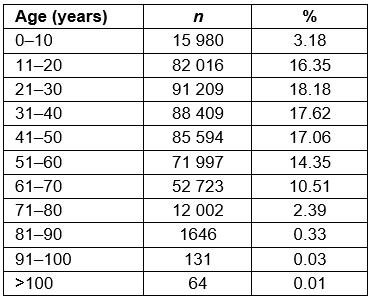
Table 2: Distribution of ocular disorders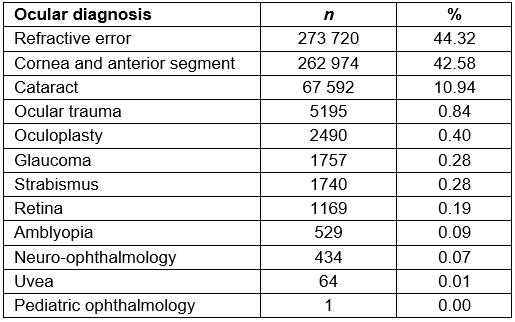
Table 3: Distribution of gender and age categories based on geographic location (state)
Table 4: Referral pattern from vision centers to secondary centers
Discussion
This study has demonstrated the demographic distribution and prevalence of ocular disorders in a large cohort of patients presenting to a three-tier eyecare network in India by using an eyeSmart app. A significant proportion of ocular disorders were in both eyes and there was no predisposition to laterality in either of them. Given the interesting gap in digitalization of eyecare services in India, this study provides an important fundamental insight into the use of a web application and tablet app (eyeSmart) to improve eyecare services in the rural areas of India. It is of utmost importance to digitize clinical information to uniformly capture the data and assess the burden of ocular disease.
To improvise the long-term health outcomes for breast cancer survivors, Baseman et al reported that the usage of the smart app is an acceptable approach in meeting the needs of breast cancer survivors (n=6) and their carers (n=4)7. Chen et al reported that use of smartphone apps is helpful in increasing the efficiency of village doctors’ work in managing children’s vaccinations in China8. In a recent study by Wong et al, 34 000 diabetic patients were screened in China for the diabetic retinopathy based on EMRs and the Messenger app9. For any healthcare intervention, apart from usage, influence on health outcomes, quality of care and experience are the major factors to be considered10.
Various mobile app-based health programs are currently in use worldwide for better healthcare services10. Access, quality and experience are the three factors on which mobile health interventions are based, to gain better health outcomes in rural areas10,11. The primary healthcare providers play a vital role in any of the healthcare services to achieve better outcomes11. In this context, the individuals who work at the primary level of eye care are the vital ones in providing better eye care services in rural areas. Hence, in this study, these individuals were well trained in the use of the eyeSmart app and its use to document clinical information of the patients. Troubleshooting and feedback of the app were communicated back to the development team by the users for timely resolution.
Various population-based studies in the nation reported that the prevalence of visual impairment in Andhra Pradesh ranged from 7.8% to 14.3%, in which the most prevalent ocular condition was refractive errors followed by cataract12-14. The present study’s findings also were similar in that the most prevalent ocular disorder was refractive errors (n=273 720, 44.32%). However, the prevalence rates of refractive error in this study are lesser than Haryana and Bhubaneshwar and greater than that of in Tamil Nadu15-19. A detailed description of these states is shown in Table 5.
The use of an app-based EMR in population health management holds promise. To the best of the authors’ knowledge, this is for the first time a tablet-based intervention using an eyeSmart app fulfilled the needs of eyecare providers working at the primary level in rural areas of India. It also provided support in providing the preliminary information to the tertiary eyecare centers through the cloud. The ability to understand the burden of disease is crucial to plan strategies to combat avoidable blindness.
The limitations of the present study include the lack of population data, patient referral bias to a tertiary care center in emerging economies and reflection solely based on the prevalence of ocular disorders and not their management. The strengths of the study include that was based on a very large cohort of patients from India. This is a first description of the prevalence of ocular disorders in a large cohort using a tablet-based application in rural areas. The tablet is portable and the app is designed to capture the vital information of various eye conditions and sync the data through the cloud.
Table 5: Prevalence rates of ocular conditions and visual impairment in other studies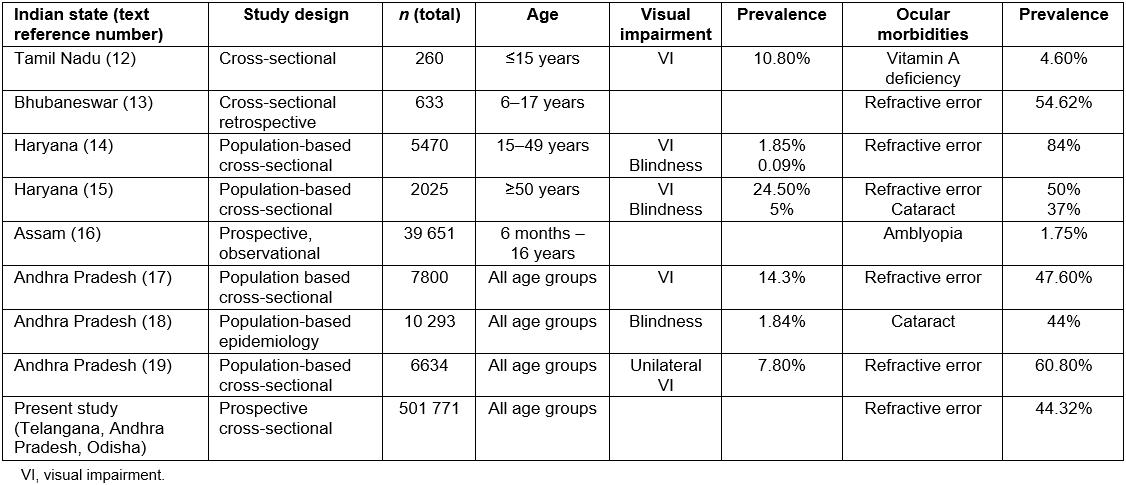
Conclusions
The present study gives detailed demographic distribution and prevalence of ocular disorders in a large cohort of Indian patients and demonstrates the potential for real-time analytics through the use of EMR systems. This provides rigorous evidence for the community and eyecare providers on the use of a web application and tablet app (eyeSmart) that this app aids in providing better eyecare services in rural areas. It helps in creating government policies and improves the treatment strategies for various preventable ocular disorders in the country.
Acknowledgement
The authors wish to acknowledge the support of our Department of eyeSmart EMR & AEye team, especially Mr Yasaswi Leela Ram and Mr Mohammad Pasha. The authors thank Mr Arjun Pola, Ms Tania Jain and Mr Vinil Ranga, who helped develop the first prototype of the eyeSmart App. The authors also acknowledge the support of Mr Uday Kumar Addepalli, Mr Karthik Sangewar, Dr Giridhar, Mr Niranjan Kumar, Dr Srinivas Marmamula, Mr Jachin Williams, Mr Surrender and the entire ICARE team who helped with the implementation of the app in the network.
References
You might also be interested in:
2014 - Knowledge and perceptions of Chagas disease in a rural Honduran community