



Introduction
eHealth technologies are often promoted as a means to improve health inequities between and within rural and remote communities. The integration of eHealth into healthcare delivery introduces opportunity for more efficient health systems, enhanced quality of care, and increased access to care for rural and remote communities. Rural communities are encountering new realities and interfaces between the local and global. Small and seemingly geographically isolated villages have become more interconnected through technological advancements in some areas, while simultaneously being left out of other, often urban-focused, initiatives. This duality is visible in health service delivery, where eHealth technologies have the potential to improve patient services, care, and outcomes, but where technological and systemic barriers can further isolate patients, caregivers, and providers1.
Although rural communities could benefit greatly from eHealth interventions, oftentimes poor infrastructure and limited resources introduce additional challenges in the capacity and capability for successful implementation and uptake. Particularly in the allocation of funding, policy and legislation are primarily focused on enhancing diagnostic technology in hospitals instead of establishing new eHealth services2. Additionally, benchmarks for adequate internet bandwidth have not been implemented, resulting in slow or unreliable internet access in rural areas3. Rural infrastructure, namely limited power and communication lines, further inhibits the successful uptake of eHealth. In addition to the systemic barriers inhibiting successful eHealth implementation, rural practitioners’ increased workload and lack of confidence in the benefits of eHealth reduce their likelihood of accepting new technology. For eHealth technologies to be integrated successfully, the goals of eHealth interventions must align with those of patients and providers using the service1.
Although previous studies have gathered patient and provider perspectives on specific eHealth initiatives, an integrated review of how patients, caregivers, and practitioners perceive eHealth interventions has not been conducted4-10. By providing a comprehensive overview of concrete, first-person feedback of past interventions, policymakers and program developers can develop strategies for using or implementing eHealth technologies that include aspects of patient voice and provider perspectives. This scoping review will facilitate informed decisions for decision-makers regarding eHealth interventions in rural communities by combining user perspectives from numerous projects. In addition, by examining perspectives from both Canada and Australia, results can be generalized to a broader population from different health systems. This review is unique in that it explicitly places the experiences and voices of patients and providers at the forefront of reviewing eHealth policies and programs.
Methods
A structured scoping review was undertaken to identify the patient and provider perspectives on the benefits and challenges for rural eHealth initiatives in Australia, Canada, and Sweden, although this article only addresses eHealth in Australia and Canada given limited publications from Sweden. Although studies have previously identified benefits and challenges of specific eHealth projects, no comprehensive review of perspectives from all studies has been undertaken in rural communities. The scoping review was guided by the Arksey and O’Malley framework: identifying the research question; identifying relevant studies; study selection; data charting; and gathering, reporting, and analyzing results11. The researchers also followed the guidelines specified in the PRISMA-ScR guide12.
This scoping review was part of a larger project to examine rural eHealth implementation in Australia, Canada, and Sweden. Through this project, researchers reviewed literature for rural and remote eHealth more broadly, with the objective of identifying the broad scope of eHealth interventions implemented in rural areas of three similarly developed countries that have placed a priority on rural and remote health. Following the broad-based scoping review, the overall findings of the eHealth review were narrowed to only literature where patient and/or provider perspectives were presented. Because the broader eHealth scoping review included all relevant eHealth studies in Australia and Canada, the eHealth database included all studies involving patient and provider perspectives that met the search criteria. Thematic analysis of articles and direct patient/provider quotations were then undertaken to synthesize and report on the resulting literature. The results were then collated, summarized, and reported.
Key terms
The terms ‘eHealth’, ‘telehealth’, ‘telemedicine’, and ‘digital health’ are often used interchangeably, with all terms generally referring to the electronic means of receiving or giving care, such as the use of video-conference or digital imaging technology13. In this article, the term ‘eHealth’ will be used consistently to denote the remote diagnosis and treatment of patients through technology. The focus for eHealth in this review is on the provision of care and does not include other aspects of eHealth such as electronic health records, robotic surgery, or blockchain developments. Common eHealth interventions include a combination of video-conferences, telephone calls, and remote monitoring devices. The term ‘rural’ is used to denote remote and regional health care14. Healthcare providers include allied health professionals and medical professionals.
The term ‘patient perspective’ is used throughout the article to denote any feedback given from the healthcare user’s point of view15. For example, the opinions or experiences of parents, caregivers, aides, or case workers may be included. Because their views reflect the experience of the patient, they are all considered together. Similarly, the term ‘provider perspective’ is used throughout the review, reflecting feedback from individuals using eHealth technologies for the provision of care.
Identifying relevant studies
Publications were initially limited to Canada, Australia, and Sweden, as these countries have universal health coverage, similar geographies, and similar challenges in rural health service delivery16. Only studies published in English inclusive of 2000–2018 were included. Concurrent searches were conducted in PubMed, Web of Science, and Scopus.
First, the broad scoping review began with a search for rural eHealth research, both qualitative and quantitative. In the search using Web of Science, key words included ((((('eHealth' OR 'telehealth' OR 'tele-health' OR 'tele-medicine' OR 'electronic health')) AND ('rural' OR 'remote')) AND ('Canada' OR 'Australia' or 'Sweden'))). Duplicates were removed, then exclusion criteria were introduced. Exclusion criteria included systematic or scoping reviews, electronic health records or documentation, general screening techniques, and unrelated technology (ie to help social work). Second, two researchers completed a title screening process in Web of Science, PubMed, and Scopus. Following the title search, results from the three databases from both researchers were pooled. Third, abstracts were reviewed. In addition to limiting results based on previously stated inclusion criteria, additional criteria were introduced. Only retrospective studies of eHealth implementation were included in the search. Hypothetical studies, for example to show a certain product would be efficient, were excluded, in addition to technological and financial evaluations. Fourth, two researchers read the full articles, using the same inclusion/exclusion criteria as in the previous levels of screenings, conducting thematic coding as articles were reviewed. Finally, when all publications of eHealth initiatives in the three countries were identified, articles including patient or provider perspectives were flagged and results from Sweden (two articles) were excluded). A separate database was created, only including the articles that included first-person perspectives from either patients, caregivers, or providers on eHealth interventions.
Classification of data
To organize and chart the data, thematic coding was conducted. Studies were classified based by relevant criteria, including type of intervention, age of target population, geographic location, and type of study. The first-person perspectives of patients and providers were then collated, and prevalent themes were identified from article text and included direct quotations. Themes were divided into positive and negative aspects of eHealth initiatives. Overall opinions of eHealth were determined by comparing the amount of positive and negative feedback provided by patients or providers. Each article was studied individually and, if the overall view of eHealth was noted to be favorable, the overall feedback was deemed positive.
The primary attributes for eHealth identified from the review were effective technology, increased support, decreased travel time, increased access to care, time and cost savings, increased patient involvement, and other. Each theme was further divided into subcategories based on prevalence of reports within the reviewed articles. When the data was categorized, a master chart was created to denote the number of articles within each category. Data were separated based on intervention type and overall feedback from patients/providers. Outcomes between different intervention types, such as tele-oncology and tele-dermatology, were also compared. Specific quotations from individuals were extracted from the articles, particularly from individuals who offered implementable suggestions to improve the program and/or constructive criticism that could be used to ameliorate future challenges.
Results
Scoping review
The primary search produced 451 results in Scopus, 578 in PubMed, and 210 in Web of Science (Fig1). Titles were reviewed and assessed for eligibility based on their relevance to rural/remote health and telemedicine, as per the inclusion criteria. Following the screening, 193 results from Scopus, 225 from PubMed, and 188 from Web of Science were deemed eligible. The results from the three databases from both researchers were pooled and duplicates were removed, leaving 311 eligible sources. The results were compared and agreed upon between two researchers at each stage of review. Following the abstract review, 181 records were deemed eligible and 130 were excluded. Following the full text review, 163 remained. After all eligible eHealth articles were compiled, the articles were narrowed by patient/provider perspectives. Due to only two publications in Sweden, the search criteria were reduced to only Canada and Australia. This resulted in 69 articles deemed eligible for review, limited to Canada and Australia.
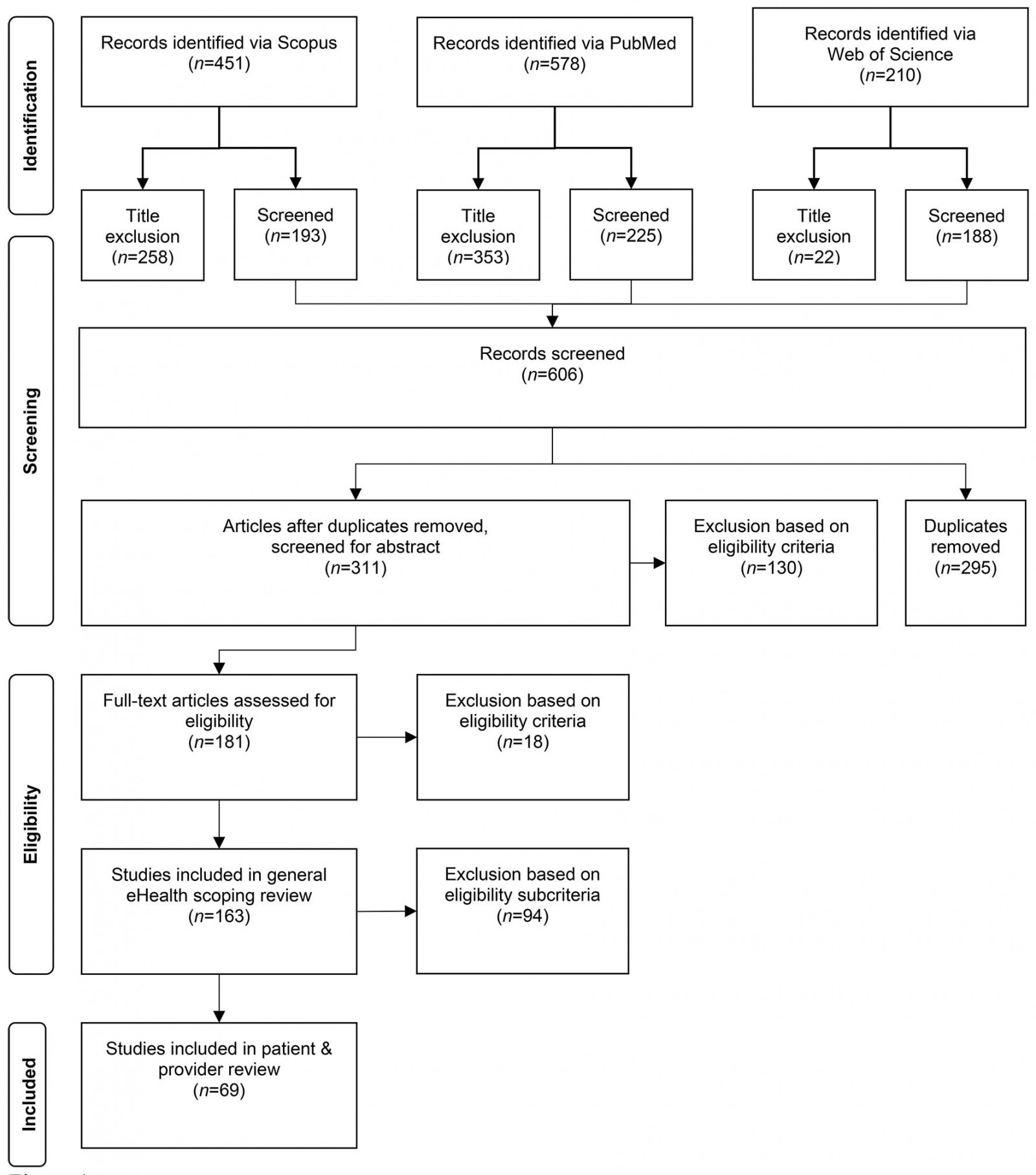 Figure 1: Adapted PRISMA flow diagram of scoping review process.
Figure 1: Adapted PRISMA flow diagram of scoping review process.
Reported benefits
The majority of articles reported positively on eHealth initiatives, at a rate of 90.1%. Only 4.2% of articles had negative views of telemedicine, while 5.6% reported mixed positive and negative views. This suggests a bias in reporting, where positive aspects are more reported in the literature and negative aspects are minimized. Thus, to gain an improved understanding of eHealth benefits, the benefits and drawbacks of eHealth were categorized and subcategorized based on prevalence in reports. The primary benefits of eHealth included decreased travel time, increased access to services, time and money saving, followed by effectiveness of technology, increased support, and increased patient involvement. Classification of these is shown in Figure 1.
Decreased travel time: Decreased travel time was the most frequently reported benefit of eHealth across all articles included in the review. In some cases, patients would have traveled 300–6500 km to attend a doctor’s appointment17. By decreasing time spent traveling, eHealth improved quality of life of patients and caregivers. Traveling to and from appointments took away time from family, from work, and from community involvement for both patients and caregivers18. Cancer patients were especially positive, as they could maximize and benefit from the short times when they felt well instead of spending it traveling to and from appointments10.
By the time we get there today [traveling 5 hours for a specialist appointment], Mum will be flat out exhausted, then when we get home tomorrow, she will be bedridden for two days to get over it [the travel]10. (patient perspective)
eHealth helped families maximize their time together and facilitate increased pleasure in periods where patients felt well. Not only the travel time but the travel itself can have negative effects on health, where patients can be exhausted from travel and take longer to recover.
Providers also reported their relief at decreased travel. Without telemedicine, doctors had to travel between rural clinics to deliver care. eHealth has enabled providers to better support their metropolitan areas while increasing engagement with rural areas19.
Access to services: eHealth has increased access to health care for both patients and providers, although the two groups have benefited in different ways. Patients reported increased access to doctors and specialists through telemedicine, while nurses and providers benefited from accessing new, diverse support services. Even when rural areas have family doctors available, the possibility of accessing specialist services within the region is limited or non-existent.
It gives them access that other [patients] that are in more densely populated areas have and they don’t miss out because of their remote location20. (provider perspective)
eHealth provides increased access to specialist services in rural and outreach areas in an efficient and timely manner to support patients in ways clinicians could not21. eHealth has also been shown to increase adherence to follow-up, particularly for youth22. By facilitating regular access to specialists, patients have found their health problems have been addressed and identified earlier than before23.
I think it’s good to really get help faster and not have to travel great distances to get the help. That’s what I find best about telehealth. Sometimes you can avoid problems by getting to them sooner. I think telehealth in general is a great thing. It’s a real advantage24. (patient perspective)
In addition to providing an increased number of services, telemedicine prevents cancellation of appointments based on transportation factors such as weather, car troubles, and length of travel to25. By increasing access to care, rural health system users reported increased education about specific issues, particularly those that are not widely recognized in small rural communities. For example, despite a high prevalence in some remote areas, diseases such as fetal alcohol spectrum disorder (FASD) are not routinely identified. Increased awareness of needs and preventative measures facilitated earlier initiation of treatment and/or prevention of disease26.
FASD isn’t as recognized in rural areas. Having FASD telehealth education available in rural communities could help get information out to everyone and let them know it’s available26. (provider perspective)
Time and money savings: eHealth has been shown repeatedly to save time and money for both patients and the health system. A study concerning an Australian tele-optometry service in rural Australia found the program would save the health system about $400,000 per year in travel subsidies alone27. The program also reduced the need for a traveling doctor, which saved $10,000 per week in addition to retaining doctors in their metropolitan areas27.
I didn’t have to travel, I didn’t have to give up a day’s work to take him [my son] somewhere and then have to worry about where I’m going to make that day’s wage up. I didn’t have to worry about what I was going to do with the other three kids, or do I pull the whole four of them out of school just to take one child to a therapist. It’s positive … he’s not distressed because he’s had to get car sick travelling somewhere, it hasn’t put a big spanner in the works of the family day-to-day routine. Just to drive to [the clinic] and back is $80 in fuel. It’s a lot of money22. (patient perspective)
Increased level of primary care and follow-up rates can also decrease hospital admissions, thereby reducing avoidable health system expenses. Telemedicine initiatives reduced inappropriate referrals or transfers to urban centers, while enabling rural practitioners to provide post-operative care following hospital discharge28.
Rural healthcare providers reported an increased level of confidence and broader skill set by observing specialists28.
It’s really good, it works really well … It also gives me an opportunity to learn as a junior doctor10. (provider perspective)
The periods of observation enabled rural providers to intervene in more patient cases, therefore reducing the burden formerly placed on specialists. After observation, the rural carers felt they could better ‘do it themselves’29.
The preparatory work before meeting with the specialist via eHealth also expanded professionals’ roles to ensure time spent in the appointment was used efficiently. The increased level of preparation led to a shorter appointment30. Patients also reported decreased wait times.
I didn’t have to sit around and wait or anything. By the time I had filled in the hospital forms and walked into the room they had already made the connection. So, it was faster, I thought it was great10. (patient perspective)
Without telemedicine, arranging an appointment with a specialist would involve weeks or months of waiting. eHealth enabled patients to avoid waiting for appointments and overcrowding of physician schedules, which was noted to have the added benefit of more cheerful patients31.
Effectiveness of technology: Positive reports of the effectiveness of technology included the ability to see, hear, and understand via video-conference. Many patients and providers were pleasantly surprised by the quality of the technology, such as high-resolution imaging and the feasibility of use. Providers noted that clear images gave them the ability to zoom remotely, with visual checks as good or even better than the naked eye32. At first, many patients thought the eHealth technology was intimidating, either because of little experience with electronics or hesitance to use it in a healthcare setting. Many reports highlighted the increasing comfort with technology after repeated use.
To start with I wasn’t confident but as I come to most of the sessions, I got a lot more confidence in it [the technology]20. (patient perspective)
High-quality technical support was an important facilitator of successful telemedicine initiatives. When technology personnel were on site, reports indicated increased satisfaction and decreased frustration with technology33.
Increased support: Patients and providers alike reported increased support using telemedicine compared to regular practice. Through videoconferencing, patients reported a more concrete support network, partially due to an improved relationship with physicians. Increased, regular contact between patients and providers facilitated rapport and created a more relaxed environment. By allowing patients to stay closer to home for appointments, eHealth facilitated the presence of family members and supporters when patients attended appointments and received treatment.
If I visit them [in the urban center], then I wouldn’t be able to explain a lot of things or have my nurse [from the long-term care facility] or daughter with me … It helps the patient a lot when [I] have a nurse or somebody there who knows what’s really going on34. (provider perspective)
The presence of family members and, when applicable, school personnel, during consultations facilitated implementation of treatment recommendations. By participating in planning process, the follow-through of recommendations was more effective22. Especially with pediatric cases, facilitating family engagement lessened the familial burden of disease. The stability and wellbeing of the family unit could remain a priority with telemedicine, due to increased time spent together and inclusion in the recovery process18.
Patients reported increased comfort and reassurance throughout the consultation when local health professionals were present. By explaining results and facilitating conversation, active participation of health professionals was a significant benefit to eHealth35.
I felt that the way the doctor had a nurse assigned to us was a plus. Her being in the room made me feel more comfortable. I knew that I could ask her anything afterwards if you had sort of skipped over something that the doctor brought up35. (provider perspective)
eHealth strengthened relationships between the local hospital, the urban hospital, and the referring general practitioner25, in addition to increased inter-agency and inter-sectional communication36.
It has been great. The opportunities with education with eLearning and [video-conference] education have been great for staff. For multi-campus facilities, it saves a lot of travel time with [video-conference] meetings, discussions, etc. that before we would have had to travel to37. (provider perspective)
Providers reported confidence in evaluations due to increased professional support, namely from specialists, in diagnoses. By creating a network of providers to seek guidance and to provide support, best practice was improved, and better interpersonal relationships were formed. Providers reported that colleague relationships strengthened, while their sense of isolation decreased38. The resulting increase in team meetings and peer support improved patient care37.
You’re able to connect with everyone involved [using telehealth]. You’re together as a team, all hearing the same information26. (provider perspective)
eHealth also improved consistency and continuity in patient–provider relationships. Often, rural health system users found it difficult to maintain a rapport with physicians. The high rate of physician turnover coupled with appointment cancellations (often due to transportation issues) made it difficult to see the same doctor or therapist33.
Communication: Patients reported increased willingness to share information with providers when using technology, particularly in the mental health sector, and facilitated communication with providers. Patients – particularly teenagers – felt more comfortable sharing personal information in the more informal format of a meeting via video-conference. Patients also felt autonomous in maintaining their own health, due to increased involvement in care.
I was in counselling and at that time, I wasn’t very comfortable with seeing [a therapist] like face-to-face, in person, until we started going on telemedicine. So, I got a little more comfortable saying what I wanted to say39. (patient perspective)
In some interventions, technology facilitators or local health professionals were available during the eHealth appointment to explain diagnoses in lay terms, which increased patient understanding26.
It just made you feel more comfortable to know that someone in your town, when you are so far away from the specialist, knows your history right through because at first you are scared about any little thing and having someone in your local area that knows your history makes you feel a lot more comfortable35. (patient perspective)
When using technology, some providers and patients felt that it was more difficult to interrupt one another, which enabled better listening40.
Reported disadvantages
Despite most articles noting overall positive perceptions of eHealth interventions, there were many disadvantages discussed in the reviewed articles. The primary disadvantages of telehealth identified were technological issues, lack of face-to-face contact, limited IT training, lack of urban–rural coordination, confidentiality, and system cost.
Technological issues: The primary reported disadvantage of eHealth was difficulty with technology. Providers reported inadequate training to use the technology efficiently, while patients reported lack of IT support. Poor internet access from undeveloped infrastructure and weather-induced shortages resulted in appointment cancellations20.
[We] don’t have the technical know-how for using IT service delivery and there is a need for better supports in place to use this technology41. (provider perspective)
Poor image resolution was a common complaint, particularly in dermatology cases42. The poor photo quality led to problems in visual acuities, which compromised the physician’s ability to get a clear picture. Users attributed inadequate picture quality to lack of training or effort27. The technological issues raised questions of the reliability of eHealth, particularly in the case of an emergency37.
Preference for face-to-face contact: The preference for face-to-face contact and/or in-person contact varied between individuals, places, and specialties. Patients that were illiterate, hard of hearing, or undereducated found it more difficult to execute appointments with technology. Older members of communities were hesitant to use eHealth services but noted that:
Down the road it [eHealth] will probably work10. (patient perspective)
Providers felt it was difficult to break bad news to patients when they were not in-person, such as explaining a poor prognosis, or to note the subtle cues that could help them with a diagnosis25. The emotional cues that are only present in personal interactions made it difficult to note small changes in a patient’s demeanor, which sometimes made thorough understanding of a situation or diagnosis more difficult38. In mental health cases, providers also voiced their concern regarding the importance of human contact in the recovery process43.
Although most individuals preferred face-to-face contact, many individuals acknowledged that they understood the importance of telemedicine and would continue to take use its services.
I am 66 years of age and used to be seen face-to-face but realise we must bow to progress25. (patient perspective)
Occupational therapists reported that telemedicine could not fully replace face-to-face, in-person assessments, but it was a good way to deliver intermediate care, such as pre- and post-operative management. Many patients and providers agreed that if the first appointment occurs in-person, then technology could easily be used for follow-up appointments.
What would be the most important thing to me is that you may be able to avoid the second visits. You know do all your tests and have the face-to-face when you have the results of all the tests, so you could avoid that second visit, coming all that way back in just one week’s time10. (patient perspective)
Speech pathologists reported that while some consultations could not be done via telemedicine, such as feeding assessments, other services were feasible through technological means44. One speech pathologist reported:
I don’t think the electronic system will ever, ever replace a heart-to-heart, face-to-face, eyeball-each-other across the table type approach to [healthcare]41. (provider perspective)
Lack of urban–rural coordination: Coordination between the referring physician and the urban practitioner introduced challenges in the uptake of telemedicine. Although referrals from rural providers for eHealth appointments with urban providers are relatively simple, patients reported that the referring provider was often not included in the conversation with the specialist. The disconnect of the rural physician introduced issues of communication and continuity of care. The frequent turnover of physicians in rural areas also added to this burden, as patients were required to re-explain their medical history each time they had an appointment45.
When the kid needs help, what the [consulting] psychiatrists are getting is a before taste, but [they] don’t get the rest of it. An evaluation – that’s the starting point – but if the kids need psychiatric treatment, there is none locally. They [the psychiatrists] make recommendations, but there is no follow-up18. (patient perspective)
In some instances, case managers, pharmacists, or local providers did not agree with the recommendations from the specialist or urban doctor. The refusal to prescribe or fill prescriptions concerned patients, leading to distrust of both the urban and the rural doctors. Additionally, the recommendations for services, such as a specialist service, were occasionally not available or were in short supply, which created unrealistic patient expectations22.
I [had] to wait for the chemo to arrive and last time, because they don’t realise that we have limited services out here [600 km away] it took five days to get here35. (patient perspective)
In an optimal situation, both physicians should be available and easily contactable to keep communication open between rural and urban centers46.
Other concerns: An important concern of some patients regarded infringements of privacy. For example, in a room of individuals receiving dialysis treatment, an eHealth appointment could be overheard by many other patients41.
I tried it and I didn’t feel comfortable talking on there because I feel like a [staff person] would hear what you’re saying … she closed the door, but I still didn’t feel comfortable with it33. (patient perspective)
Although the concern for privacy was expressed by many healthcare users, it was also noted that the risk of privacy breach was not any greater than that of a regular in-person doctor visit44.
Discussion
eHealth has become a prevalent topic of interest and of study among health professionals, health planners, and policymakers at all levels. It has been identified as a feasible method to improve access to health care for rural and remote communities. Although hundreds of studies have reported on specific eHealth interventions, feedback provided by patients and providers is often ignored within academic discussions. By solely focusing on the experiences of individuals using eHealth technologies, systemic and local barriers can be identified in the uptake of eHealth.
Based on the reviewed literature, it was determined that eHealth interventions are perceived as a positive means of facilitating access to health care for rural areas. However, patient and provider voices highlight areas for caution in eHealth implementation.
According to patient and provider feedback, primary advantages of rural eHealth include decreased travel time, increased access to care, and time and cost savings. These advantages are prevalent across all specialties and are reported by patients and providers alike. The primary disadvantages of eHealth include technological issues, lack of face-to-face contact, and lack of coordination between urban and rural providers. Technological issues impede successful use of eHealth due to inadequate internet access and ineffective technology. Despite the positive feedback regarding eHealth, successful implementation is inhibited by substantial disadvantages – most notably by the lack of affordable, reliable technology and of adequate internet access.
To effectively improve eHealth interventions, the drawbacks identified by patients and providers must be addressed. The primary barrier to the successful uptake of eHealth is inadequate technology, which would require larger scale planning and support to successfully reform. The issue of inadequate internet access should be at the forefront of eHealth development; however, the importance of providing reliable internet access is not fully understood by policymakers. A framework for successful internet and electronic outreach should be developed in order for eHealth to be successfully integrated into the healthcare system, in addition to a greater understanding of the long-term financial implications of such changes.
Although addressing the need for technological advances requires a larger network of support, local changes can also greatly ameliorate eHealth satisfaction and success. Facilitated communication between urban and rural providers would increase continuity of care and provider satisfaction, while decreasing patient confusion. With better communication, urban providers would be more informed regarding available services in rural areas. This knowledge could mitigate potential frustration if recommended treatment options are not available in communities. Additionally, the presence of a local nurse or healthcare provider during eHealth consultations would alleviate patient confusion and discomfort.
The literature strongly suggests that patients and providers regard eHealth as an asset. However, it is important to consider the tendency for journal publications to favor positive reports of eHealth. Undertaking further research to better understand the first-hand experiences of eHealth interventions would provide a more complete understanding of the successes and drawbacks of the service.
Study limitations
Scoping reviews are limited, as relevant sources may be omitted based upon the availability of studies related to the research question. To mitigate bias, this scoping review was conducted by two researchers to standardize inclusion and exclusion criteria. Additionally, in scoping reviews, the quality or level of evidence of the studies are not taken into consideration. To expand upon this review, a more thorough investigation of the quality of each article could be undertaken.
Conclusions
This scoping review provides a unique perspective on eHealth implementation in rural and remote communities through the prioritization of first-person voices from patient, caregivers, and health providers. Within scoping reviews, the voices of individuals are often lost, with primacy placed on the conclusions of academics in published articles. Through interpreting the feedback from individuals in a broad manner, a more nuanced impact of eHealth can be drawn, as well as the recognition that health care, even when through digital means, is inherently based on person–person relationships. This perspective also fits with that of rural health in general, where small communities and strong social connections are defining features of rural life.
The results of this review highlight the many advantages of rural eHealth, but also note that there are systemic and technical barriers for implementation. A major limitation to expanded rural eHealth is coordination at regional and national levels for expanded high-speed internet. It is noted by patients and provider alike that rural communities are being isolated through inadequate and unreliable internet connectivity. In the case of rural eHealth, this translates into a safety and equity issue, not just inconvenience.
At a local level, providers and patients appear more than willing to adopt eHealth technologies. Numerous benefits are noted in the literature, even if some patients reflect on initial hesitations. These benefits extend beyond just access, where successful interventions see secondary benefits such as improved support, consultations, and learning opportunities for providers; and more cohesive care, improved understanding, and timely appointments for patients and caregivers.
An additional finding from this review is that the ancillary benefits to patients and caregivers are as important as those that are directly quantifiable. Qualitative discussion notes that having local access to appointments reduced anxiety and stress associated with travel and allowed patients to stay close to home. Families were impacted less from eHealth appointments, with children able to stay in school, parents and partners not having to take additional time off work, and patients noting quicker recovery.
Based on this qualitative review, future directions for eHealth should include a concerted push for regional and national high-speed internet access networks. However, this alone is not enough – there needs to be additional training and support for implementation of new eHealth technologies at the local level, where rural health providers need to be trained in the technicalities of setting up and maintaining these systems.
Local sites need to remain flexible and adaptive, where the many uses for eHealth must be integrated into single end-user systems. In small communities, having one site that can provide remote diagnostics, practitioner eLearning, specialist consultation, mental health services, and the like would minimize system costs, reduce the need for practitioners and patients to learn many systems, and enhance the utility of rural eHealth across the healthcare system.