

Introduction
Oral diseases are among the most prevalent diseases worldwide, with dental caries, periodontal disease, edentulism and oral cancer being the most common1. The presence and progression of these diseases can cause social and economic problems at the individual, household and health system levels, with the consequent increase in inequalities that mainly affect vulnerable populations1. One of the most affected population groups is children from developing countries living in poverty and extreme poverty, especially those with low access to dental services1. The current global oral health landscape has promoted the launch of an urgent call to prioritize global public health care for oral diseases, with a focus on reducing inequalities2.
The most prevalent oral diseases in children are caries and periodontal disease. In developing countries such as Peru, poor epidemiological information at the population level shows that tooth decay reaches prevalences of 70–90% and for periodontal disease 75–80%3,4. More recent studies in targeted populations show that these prevalences remains constant5-7. In Peru, a set of public health actions have been implemented to reduce these diseases at the population level8,9. However, these strategies have not shown the expected results in light of the high prevalence of oral diseases. This is possibly due to an ineffective promotion of preventive methods, little awareness of oral health care, and a predominance of recuperative and cosmetic treatment preferences by dental professionals and users of dental services.
In the dental office, the measures of prevention of caries and periodontal disease that can be applied from the eruption of the first tooth are the application of sealants of pits and fissures, dental prophylaxes and the application of topical fluoride. However, in Peru, where access to dental services in the population of children does not exceed 24%10, these measures should be complementary to adequate oral hygiene practices at the individual level, by brushing (two or more times a day) with fluoridated toothpaste, changing toothbrushes after 3–4 months of use, and not sharing toothbrushes, which are recommended and backed by national and international oral health agencies11-13. Failure to follow these recommendations could compromise the effectiveness of these measures to prevent tooth decay and periodontal disease.
The adoption of adequate oral hygiene practices presents differences at the population level, and in children it generally depends on contextual factors and those of the parents. Studies indicate that the caregiver’s educational level, socioeconomic status, as well as parents’ oral hygiene practices, are some of the factors that are associated with the adoption of oral hygiene practices in children14-16. Knowing these factors allows us to guide an improvement in the dissemination of preventive methods in oral health in the most vulnerable population groups. In Peru, there are large health disparities between rural and urban areas; however, it is currently unknown how this affects the adoption of adequate oral hygiene practices in the Peruvian population, considering that the rural area represents 21% (more than six million inhabitants) of the total population17.
In Peru, the Demographic and Family Health Survey (ENDES in Spanish) descriptively exposes the distribution of adequate oral hygiene practices among the population of children aged less than 12 years. However, it does not present the factors associated with the adoption of these habits, taking into account the possible differences at rural and urban levels. Therefore, the objective of this study was to evaluate rural–urban differences in the adequate oral hygiene practices of Peruvian children aged less than 12 years, as well as associated sociodemographic factors.
Methods
Study design and data sources
A cross-sectional study was conducted of 41 330 children aged 1–11 years, with complete data on proper oral hygiene and their caregivers contained in the ENDES survey. The ENDES is carried out annually by the Peruvian National Institute of Statistics and Informatics and contains information on the oral, eye and mental health of children aged 0–11 years, which is obtained by the people responsible for their care. The details of sampling, processing and collection of data can be consulted in the final technical report18.
Variables
The study variables and their respective codes were obtained from the 2018 ENDES survey. Oral hygiene practices was the dependent variable, which was considered adequate for toothbrushing two or more times a day, having a toothbrush for individual use and changing toothbrushes every 3 months. If at least one of these conditions was not met, practice was considered as inadequate oral hygiene. The following independent variables were included in the analysis: sex (male, female), age group, level of education of caregiver or head of household (no formal school, primary, secondary, higher), health insurance (yes, no), use of dental services defined as any dental care 6 months prior to the survey (yes, no), region of residence (coast, highlands or jungle) and wealth index quintiles (poorest, poorer, middle, richer, richest).
Statistical analysis
Data analysis was conducted using Stata v14.2 (Stata Corp; https://www.stata.com/stata14). Absolute frequencies and weighted proportions for characteristics of children with adequate oral hygiene and their caregivers were reported. The χ2 test was used to evaluate the association between independent variables and adequate oral hygiene. For the crude analysis, prevalence ratios (PR) and 95% confidence intervals were estimated as measures of association. Independent variables with p<0.20 in the crude analysis were included in the adjusted model. Generalized linear models of the Poisson family with link function (log) were used for crude and adjusted analysis and a value of p<0.05 was considered statistically significant. All interest variables were reported according to place of residence (urban/rural).
Ethics approval
The study did not require the approval of an ethics committee because it was a secondary analysis of the 2018 ENDES survey, for which data are in the public domain and do not identify the evaluated participants. The 2018 ENDES database is free and can be accessed at http://iinei.inei.gob.pe/microdatos.
Results
From a total of 41 330 children, 50.8% were male, 55.3% belonged to the age group of 6–11 years, for 42.7% the head of the household had secondary-level education, followed by higher (30.4%) and primary (24.1%), 84.4% had health insurance, 68.1% had not used dental services 6 months prior to the survey, 55.6% were residents of the coast, and 25.5% belonged to the poorest welfare quintile, followed by quintiles 2 (poorer; 23.3%) and 3 (middle; 20.0%) (Table 1). The prevalence of appropriate oral hygiene practices in the urban area was 57.3% (95%CI 56.2–58.3%) and 38.3% (95%CI 36.6–40.0%) in the rural area, with a difference of 19 percentage points between categories (p<0.001) (data not shown). The greatest rural urban percentage differences in the weighted proportions of the independent variables were primary education level for the head of the household (14.4% (95%CI 13.6–15.3) urban v 52.3% (95%CI 50.3–54.3) rural), no health insurance (17.9% (95%CI 17.1–18.8) urban v 9.0% (95%CI 7.9–10.2) rural), residing on the coast (69.6% (95%CI 68.6–70.6) urban v 14.9% (95%CI 12.4–17.8) rural) and belonging to the poorest welfare quintile (6.9%; 95%CI 6.4–7.6) urban v 79.3% (95%CI 77.2–81.3) rural) (Table 1).
All the variables studied showed a statistically significant association (p<0.001) with appropriate oral hygiene practices in urban and rural areas, except for the welfare quintiles of poorer, middle, richer and richest (Table 2).
In the urban residence area, the adjusted multivariate analysis showed a significant association with the adequate oral hygiene practices of the following variables: age group 6–11 years (PR 1.32 (95%CI 1.28–1.35; p<0.001)), use of dental services (PR 1.16 (95%CI 1.13–1.20; p<0.001)), residing in the highlands (PR 0.83 (95%CI 0.79–0.87; p<0.001)), residing in jungle areas (PR 1.10 (95%CI 1.06–1.15; p<0.001)), and welfare quintile categories of middle (PR 1.10 (95%CI 1.02–1.20; p=0.013)), richer (PR 1.13 (95%CI 1.04–1.23; p=0.003)) and richest (PR 1.25 (95%CI 1.15–1.37; p<0.001)). In the rural areas, all variables were significantly associated with adequate oral hygiene practices, except jungle area of residency (PR 0.90 (95%CI 0.81–1.01; p=0.068)) and the richest welfare quintile category (PR 1.31 (95%CI 0.92–1.85; p=0.137)) (Table 3).
Table 1: Characteristics of children aged 1–11 years and their caregivers, 2018 ENDES survey 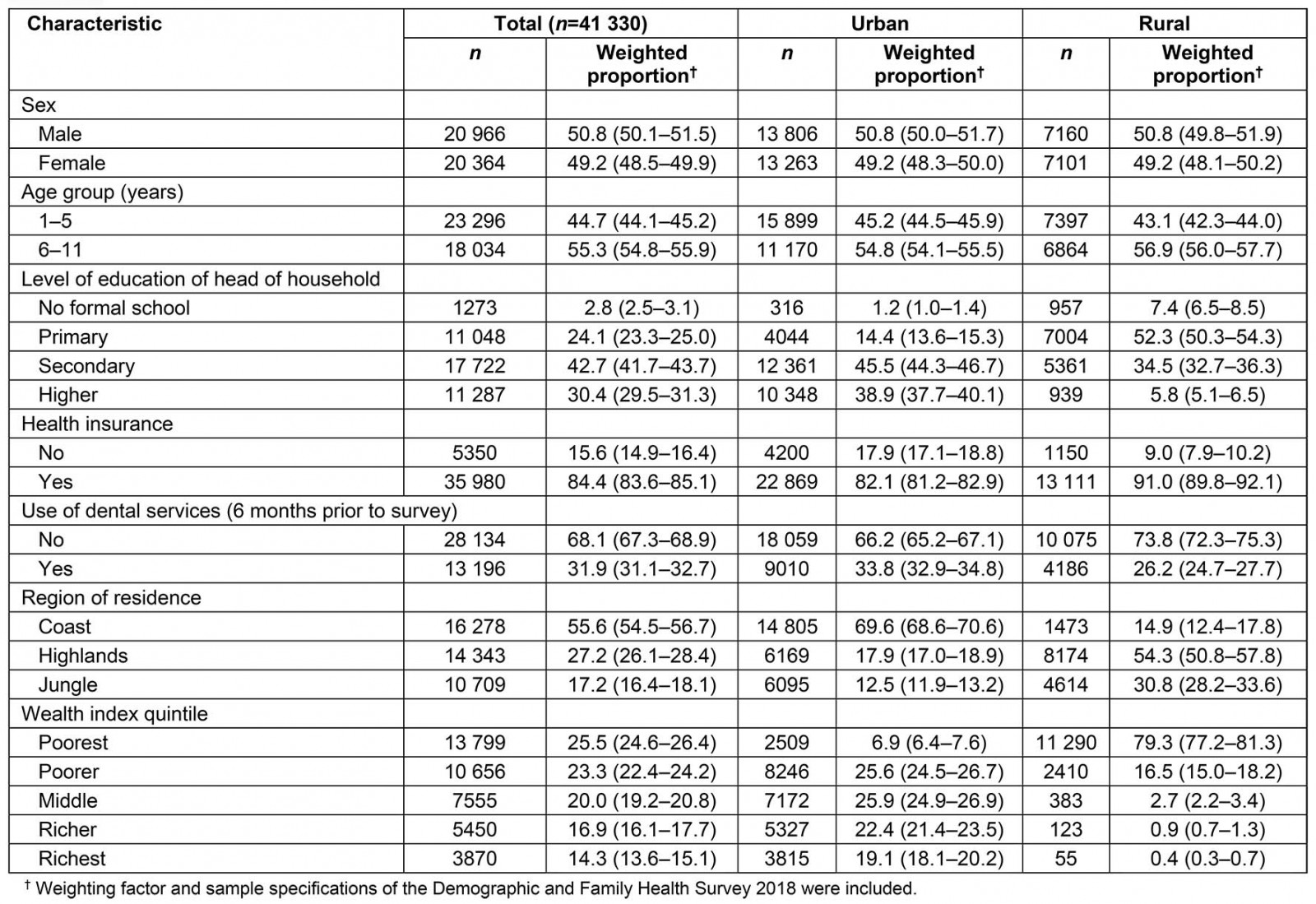
Table 2: Rural and urban differences for adequate oral hygiene practices according to characteristics of children aged 1–11 years and their caregivers, 2018 ENDES survey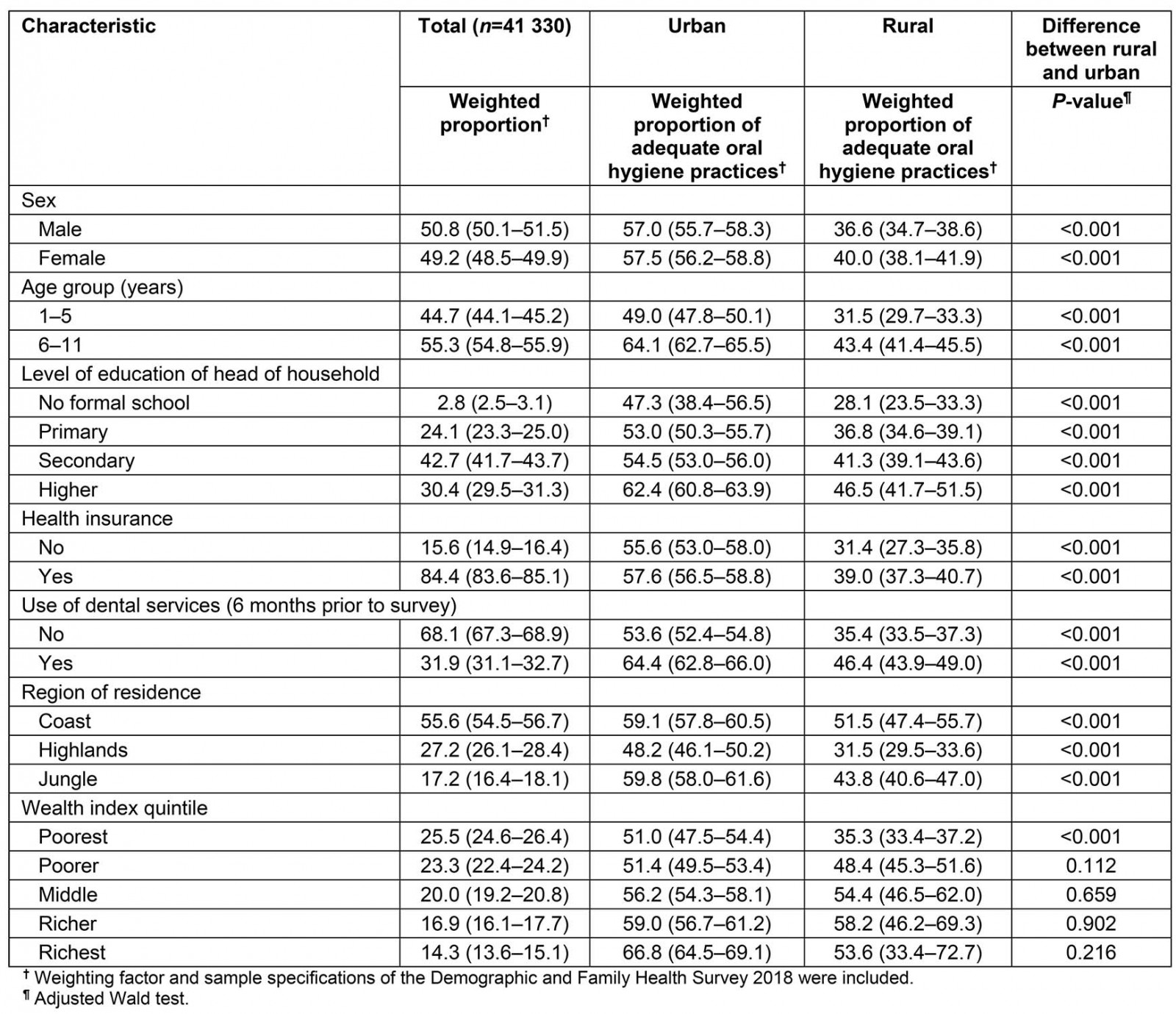
Table 3: Factors associated with adequate oral hygiene, 2018 ENDES survey†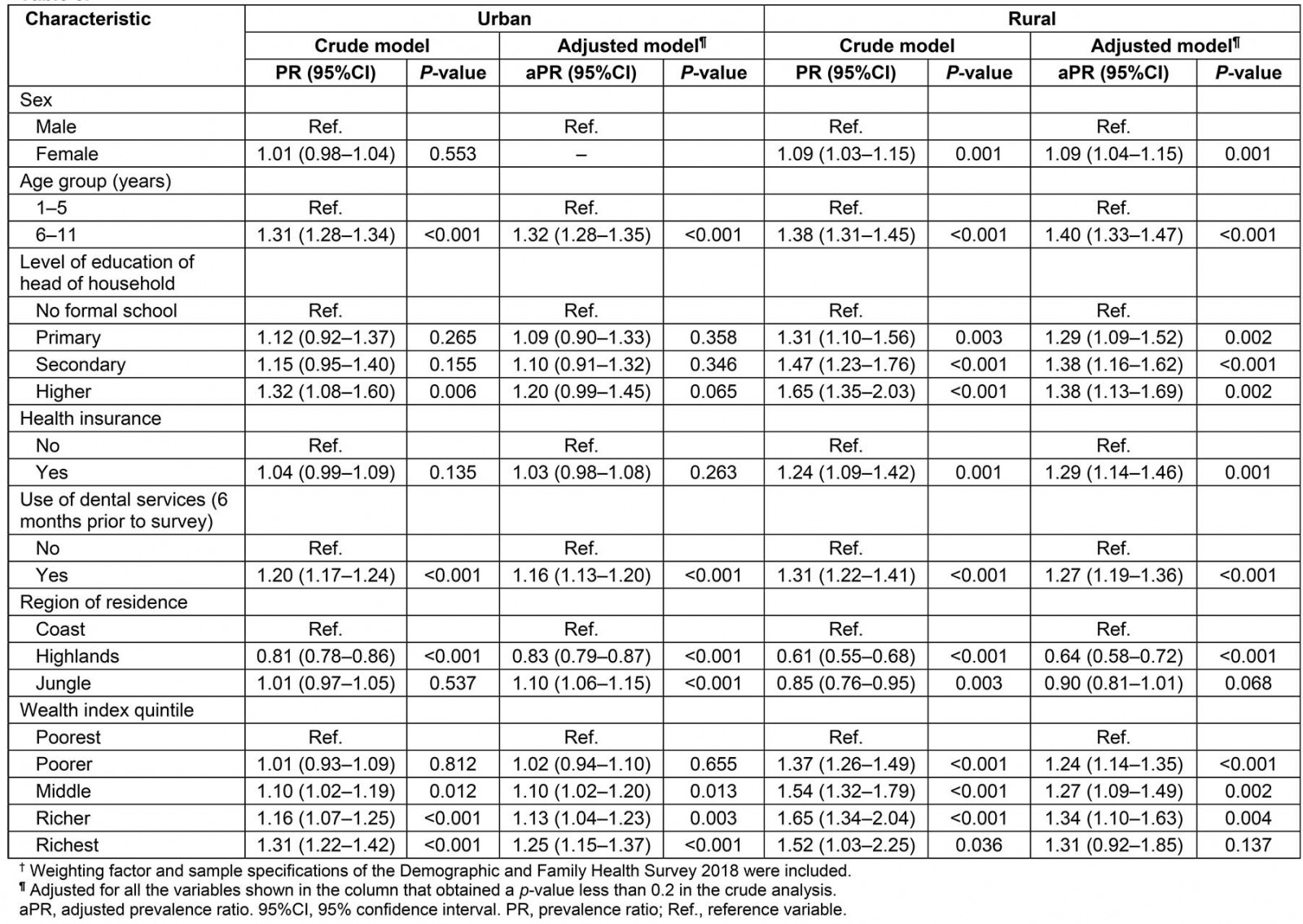
Discussion
The present study identified a lower prevalence of adequate oral hygiene practices in rural areas (38.3%), with a significant difference of 19 percentage points with respect to urban areas (57.3%). The distribution of the proportion of adequate oral hygiene practices was lower for all the variables in rural areas compared to urban ones; the biggest rural–urban differences were observed among those in the age group of 6–11 years (43.4% v 64.1%), those where the head of the household had no formal education (28.1% v 47.3%) or primary education (36.8% v 53%), those who used dental services in the previous 6 months (46.4% v 64.4%) and those residing in the highlands (31.5% v 48.2%). The factors associated with a higher probability of adequate oral hygiene practices in rural areas were being female (compared to being male), belonging to the 6–11 year age group (with respect to the 1–5 year age group), belonging to the primary, secondary or higher educational level (with respect to no formal education), having health insurance, having used dental services 6 month prior to the survey and belonging to the poorer, middle or richer welfare quintiles (with respect to the poorest welfare quintile). Also for rural areas, residing in the highlands was associated with a decreased probability of adequate oral hygiene practices (with respect to the coast).
In the present study, an association was found between being female and a greater probability of adequate oral hygiene practices in rural areas. In this regard, a study by Kamath et al showed that in the child population (6–15 years) of a rural area of India, the highest proportion of children who brush twice a day was female (78.6%), compared to male children who had the same habit (46.6%)19. In this respect, it is well known that there is a gap in health outcomes and preventive behaviors between men and women, mainly influenced by established gender norms in society20. This trend is not absent from oral health issues, even in children21, where girls have shown better preventive practices than boys. In relation to age of the child, an association was found between children aged 6–11 years and a greater probability of adequate oral hygiene practices in urban and rural areas. An explanation for the present study’s results could be that parents may have a misconception about the age when oral health practices such as toothbrushing should begin – they may believe that dental decay in the primary dentition is not important because these teeth are replaced by permanent teeth. Both sex and age are well known sociodemographic factors affecting inequalities in health outcomes such as oral hygiene practices. Therefore, these factors should be taken into account in policy development and promotion strategies for adequate oral hygiene practices.
Education level plays an important role in the adoption of habits and self-care in health. The present study reports a relationship between a higher educational level of the head of the household and a greater probability of adequate oral hygiene practices in rural areas. This finding is similar to that reported in a study from India, where the adoption of oral health habits in children was positively influenced by habits adopted by parents, as well as by their education level15. An explanation for this association could be that information on oral diseases and their preventive methods is included in study curricula at higher levels of education. It is also known that people with higher educational levels have greater purchasing power, and that this also conditions a greater use of dental services, which guarantees periodic exposure to information on oral health prevention, as reported by studies performed in populations from Iran22, India23, Chile24, and the USA25. This association is not visualized in the area of urban residence, possibly because the distribution of the population in the reference category (no formal education) is only 1.2%, while in the rural area it is 7.4%. In addition, there is greater uniformity in the population distribution in the categories of education levels in the urban area26. Because of this, there is a need to strengthen the promotion of proper oral hygiene habits in education curricula, as recommended by WHO. Furthermore, it should be taken into account that, in the rural area of the study sample, 5 out of 10 people do not exceed the primary education level, compared with 1 out of 10 in urban areas (with 8 out of 10 achieving secondary or higher education levels)27; this rural–urban settings gap in education has also been reported for the majority of Latin American countries28. For this reason, these countries also need the implementation of oral health promotion strategies at the individual level in health centers, and at the community level in rural areas.
The possession of health insurance is essential for access to health services for preventive and oral recovery of the population, mainly of low income. It is also during the care process that users receive relevant information about preventive health habits. The present study reported that having health insurance increased the chances of having adequate oral hygiene practices in rural children, which has been previously reported in a Brazilian adult population29. In light of these results, it should be mentioned that the rural population in Peru has a higher percentage of insured people than the urban area (83% v 73%)30; however, the periodic use of dental services in children under 12 years is less10. This is possibly due to a problem in the offering of treatments, low numbers of dentists and accessibility to dental services, which is common in rural settings around the world31,32. This could mean that this population is not receiving information about preventive measures of oral health, which in turn affects the adoption of adequate oral hygiene practices in children. Therefore, maximum health insurance coverage should be ensured, as well as facilitating the use of coverage for dental services in the rural settings, as well as the deployment of teams of dental professionals to provide care and promotion of oral health in remote and difficult-to-access areas.
A gradient was evidenced in the adoption of adequate oral hygiene practices with respect to welfare quintile in the rural area: the probability of adequate habits was greater for better welfare quintiles, except for the richest welfare quintile category. This is possibly due to the fact that the proportion of the population belonging to this welfare quintile in rural areas represents only 0.4% of the population. In addition, in Peru and the majority of Latin American countries, the population living in poverty has the lowest rates of educational attainment33,34, which is important because a higher education level of parents is associated with a better adoption of healthy oral health habits in children in the present study. Similarly, some studies in Peru, Nicaragua and Nigeria reported that a greater quintile of wellbeing or a higher level of parent education is associated with a greater frequency of use of oral health services in children, which is essential for receiving information on adequate oral hygiene practices10. In that sense, it is necessary that social programs focus efforts on the populations with less resources in the rural area to ensure that they receive timely information on oral hygiene habits – even more so considering that almost 75% of the population living in poverty in the world is concentrated in rural settings.
Living in the highlands reduced the chances of adequate oral hygiene practices in children in rural areas. In this regard, it is worth mentioning that the population of the highlands concentrates most of the rural population, which in turn has the highest percentages of population without education and with higher poverty rates, lower access to drinking water and lower supply of health services, factors that can affect the adoption of adequate oral hygiene practices. However, contrary to this study’s results, a study in Brazil showed that there were no significant differences between the frequency of toothbrushing in children and adolescents aged 12–17 years in the rural–urban population, although they presented a similar trend to that of the present study in the education levels of the mothers and socioeconomic level of the population35. Therefore, other factors could play a preponderant role in this association, such as the use and accessibility of dental services, low availability of dental services, as well as low exposure to promotional campaigns of hygiene habits at the community level.
One of the main limitations of this study is the use of the secondary ENDES database, which may have had some information bias by informants or interviewers, or possible errors in filling out the survey; however, the latter receive training and standardization prior to the application of the survey to reduce this possible bias. Also, because some homes may have two or more siblings, the independence of the information regarding the characteristics of the parents of the children included in the study cannot be guaranteed. Despite these possible limitations, it should be mentioned that ENDES is a survey that has national and urban–rural representativeness.
Conclusion
Only 4 out of every 10 Peruvian children residing in rural areas perform adequate oral hygiene practices, in comparison to 6 out of every 10 children in urban areas. Likewise, being female, belonging to the 6–11 year age group, having a higher education level, having health insurance, having used dental services in the 6 months prior to the survey and belonging to a greater wealth quintile were associated with a greater probability of adequate oral hygiene practices in rural areas. Residing in the highlands was associated with a decreased probability of this outcome. There is an urgent need to strengthen strategies aimed at improving oral health in rural settings of the world, taking into account the socioeconomic gradients identified between the rural–urban areas in this study and others from different countries as previously discussed. In that sense, it is necessary to complement current strategies with a greater presence of the promotion of oral health in the curricula of different education levels, and in campaigns at the level of health and community centers. Furthermore, there is a need to increase the promotion of the use of oral health services in rural settings, in order to reduce existing rural–urban inequalities in relation to access to oral health services, access to information on adequate oral hygiene practices and access to accessories necessary for adequate dental hygiene (toothbrushes and toothpaste that meet quality standards).
Acknowledgements
The authors thank the National Institute of Statistics and Informatics, which conducted the Demographic and Family Health Survey and made the dataset and report available online.