

Introduction
Life satisfaction has attracted attention in numerous disciplines1-4. Some have stated that maintaining a high level of satisfaction with life should be a priority for governments and societies5,6. While related to depression, the notion of life satisfaction is broader, and measured differently7. Life satisfaction is a subjective global measure of one’s life as a whole at the present time and differs from quality-of-life measures that include specific symptoms and impairments. Most older adults in modern societies are satisfied with their lives8-10. A recent report shows decreased life satisfaction in middle age (ages 45–54 years) and increased life satisfaction in older age groups in high-income, English-speaking countries9. A high percentage of community-dwelling Canadians over 65 years reported they were satisfied with life10. There are various measures of life satisfaction, most of which use rating scales that categorize respondents’ self-perceived level of psychological wellbeing7. Single-item questions have been shown to be as reliable as longer questionnaires in explaining variances in mortality after adjusting for other risk factors7. Factors associated with life satisfaction in community-living older individuals are frailty11, cognitive status12, overall health13, functional status14, and self-esteem15.
Interest in rural health and wellbeing has a long history, being a topic of interest in John Graunt’s mortality bills in the 1600s. Wirth speculated that urbanization disrupted traditional relationships, and this led to displaced personal relations, and institutions that catered to societal needs rather than to individual requirements16, leading in turn to differing levels of life satisfaction. Other potential factors could be closer social networks, more stable long-term relationships, less economic uncertainty, lower population density, and an established sense of community. With the continual rise in the level of urbanization worldwide17, understanding life satisfaction in urban and rural populations is important for planning social and healthcare services in rural populations. To date, the exploration of rural–urban differences in life satisfaction has been somewhat limited because few population-based surveys of both rural and urban populations consider the effect of potential confounding factors, such as income and health status. Ahn and Lee showed that poor health status was strongly associated with lower life satisfaction in rural populations, but the study was limited to nursing home residents in rural areas18. Cantarero and Potter found high levels of life satisfaction in older rural Nebraska residents, except for satisfaction with transportation8, but there was no urban comparison group. In a general population, Clark et al found higher levels of life satisfaction in rural areas than in urban regions and increasing levels of life satisfaction in rural areas over time – perhaps due to changes in public policy targeting rural infrastructure and poverty19. In a general population in Canada, Helliwell et al found that urban regions had lower life satisfaction than rural regions, although there was a substantial variability between and across both rural and urban communities9,20. In rural areas in developing countries, income was strongly associated with life satisfaction, although this effect was most pronounced at lower incomes21. While previous research has provided insights into life satisfaction in rural areas compared to urban areas, there are gaps in the understanding, since relatively few large representative studies of life satisfaction in rural populations include measures of potential confounding factors, such as health status. The authors therefore sought to explore life satisfaction in rural populations in the Canadian Longitudinal Study of Aging (CLSA), which has a large sample of rural Canadians, aged 45–85 years. The specific objectives are to determine:
- life satisfaction in rural populations of Canadians aged 45–85 years
- if there are differences in life satisfaction across a rural–urban continuum amongst Canadians aged 45–85 years, after accounting for potential confounding factors
- if the factors associated with life satisfaction differ in rural and urban populations, by looking for interactions between rurality and these other factors.
Methods
The CLSA is a population-based cohort study, which is ongoing22-24. For the present study, a cross-sectional sample from the initial survey wave of the CLSA tracking cohort was used, which was intended to be as generalizable as possible to the Canadian population of 2008. At the time of analysis, only cross-sectional data were available. The sampling frame for the tracking cohort was complex but based on Statistics Canada geographical classifications25. All dwellings within the same census dissemination area block (CB) identified as either urban or rural were grouped together. In each province, clusters of these blocks were created having a fixed number of dwellings with a minimum number of people in the 75–84 years and 85 years or over age groups. Clusters were composed entirely of urban or rural census dissemination area blocks and could not cross provincial boundaries. This sampling strategy ensures accurate categorization of rurality as well as an adequate sample size for rural analyses. Exclusion criteria for the CLSA study sample were individuals residing in the three territories and some remote regions, or residing on federal First Nations reserves and other First Nations settlements in the provinces, full-time members of the Canadian Armed Forces, individuals living in institutions, individuals holding a temporary visa or having transitional health coverage, individuals unable to understand English or French, and individuals with overt cognitive impairment. Data from all participants were collected between 2010 and 2014, using computer-assisted telephone interviewing. Informed consent was obtained from all participants.
Definition of ‘rural’
There are numerous definitions of rurality, and the definition used can influence research findings26. This study used the definitions of ‘rural’ used in the CLSA sampling frame. These are similar to the definitions used in the Canadian Community Health Survey27 and the 2006 census. A detailed description is provided in the 2006 Census Guide28. To summarize, geographical definitions are based upon the size of the community. A census metropolitan area or a census agglomeration is formed by one or more adjacent municipalities centered on a population center (known as the core). A census metropolitan area must have a total population of at least 100 000, of which 50 000 or more must live in the core. A census agglomeration must have a core population of at least 10 000. To be included in the census metropolitan area or census agglomeration, other adjacent municipalities must have a high degree of integration with the core, as measured by commuting flows derived from previous census place of work data28. The definition of rurality and the sample size within each category in the CLSA tracking cohort data are shown in Table 1. For these analyses, the definitions were collapsed into four categories: rural versus mixed (defined as the ‘postal code link to dissemination area’ variable, indicating some rural, but could also include some peri-urban areas) versus peri-urban (‘urban fringe, and secondary urban sites’) versus urban (‘urban core’). These categories allow consideration of increasing rurality across a rural–urban continuum. Because there is a large sample of rural adults, there is considerable power to detect differences in life satisfaction across this continuum.
Table 1: Definitions of ‘rural’ and ‘urban’, and sample size in the Canadian Longitudinal Study of Aging tracking cohort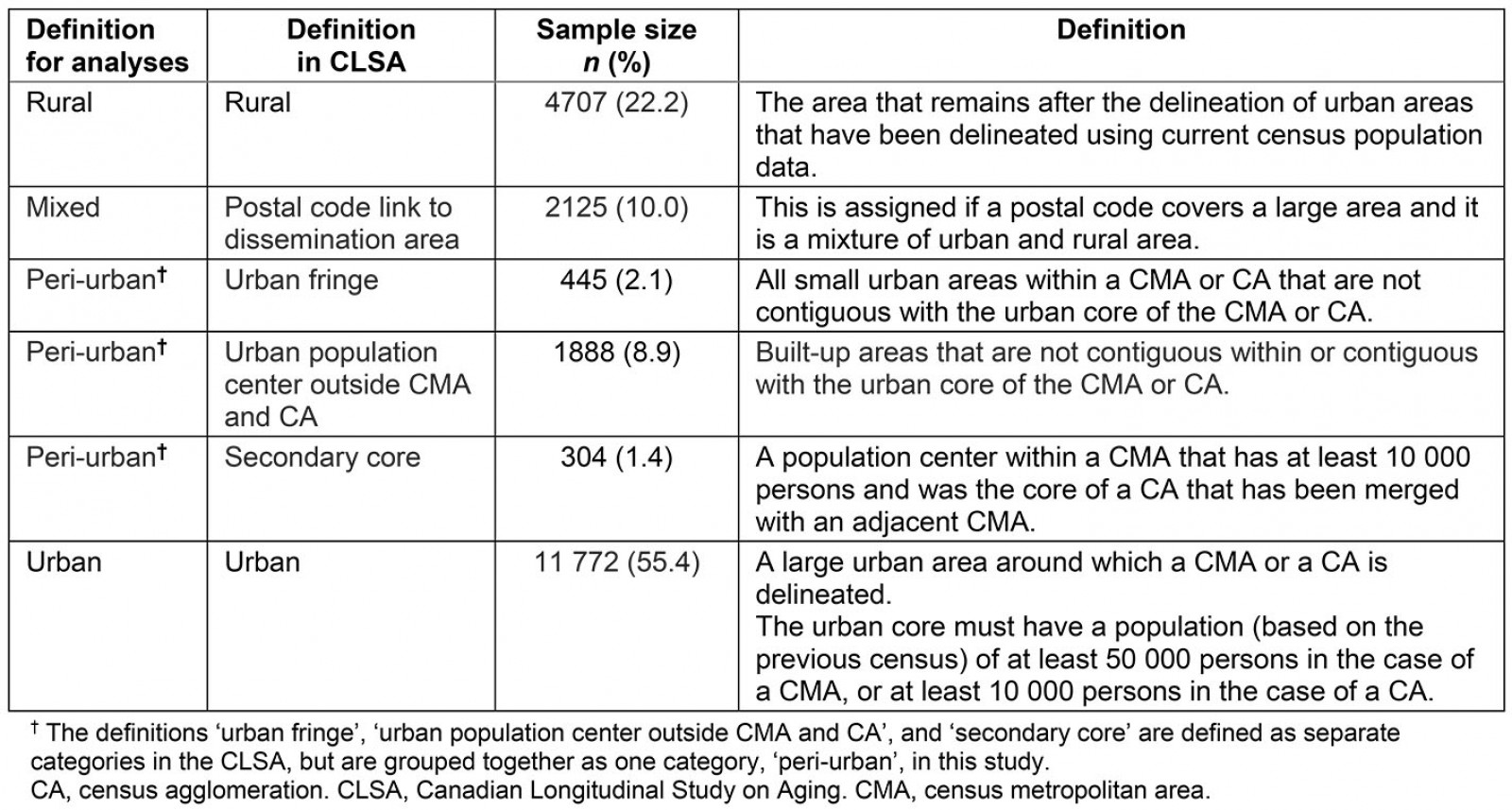
Measure of life satisfaction
The CLSA used the Satisfaction with Life Scale to measure life satisfaction29,30. This is a widely used global measure of life satisfaction that has established reliability and validity, and that has been translated from English and adapted for use in French. There are several items: ‘In most ways, my life is close to my ideal’; ‘The conditions of my life are excellent’; ‘I am satisfied with my life’; ‘So far, I have gotten the important things I want in life’; ‘If I could live my life over, I would change almost nothing’. The summed score range is 5–35. In this study, the score was not normally distributed, with most participants being satisfied with life. Therefore, the score was dichotomized into those who were satisfied (scores 26 or more) and those who were dissatisfied with life (scores less than 26). In the CLSA cohort, participants who scored 26 or higher were considered satisfied, while participants with a score of 31–35 were extremely satisfied. An indication of scores less than 26 ranged from being extremely dissatisfied to being slightly satisfied with life31.
Other factors considered
A number of potential confounding factors and interactions were considered in the analyses. Sex was grouped into two categories (‘male’ versus ‘female’), education was grouped into four categories, household income was considered in categories of <$20,000, $20–49,999, $50–99,999, $100–149,999, and >$150,000, all in Canadian dollars; living situation was considered in two categories (‘alone’ versus ‘not alone’); and marital status was categorized as ‘never married’, ‘married/common-law’, ‘separated’, ‘divorced’, and ‘widowed’32. In addition, self-reported chronic conditions were considered. These conditions were less likely to be subject to surveillance bias due to differential access to health care in rural areas compared to urban areas33: Chronic obstructive pulmonary disease, stroke or cerebrovascular accident, ischemic heart disease, cancer (any site), osteoarthritis, and cataracts34.
Analysis
To account for the complex sampling design, the CLSA has calculated weights to create prevalence estimates that represent the Canadian population (inflation weights) and for estimating associations (analytic weights)35. Analytic weights are inflation weights that have been rescaled to sum to the sample size within each province. Both weights were provided in the CLSA data set. Descriptive characteristics considered the inflation weights, while analyses included the analytic weights. Participants for whom data were missing for residence or for satisfaction with life were excluded. In addition, in statistical models, those with missing variables on the confounding factors were excluded.
Bivariate analyses were conducted using χ2 tests for categorical variables. Since the life satisfaction measure was not normally distributed, with most participants having high levels of life satisfaction, life satisfaction was dichotomized into ‘satisfied’ and ‘dissatisfied’. Then, logistic regression models were constructed with the outcome of life satisfaction. A series of models were constructed beginning with adjustment for age and sex, then for the remaining sociodemographic factors, and finally for health-related factors. Per CLSA recommendations36, analytic weights were considered, and province of residence was included in all regression models (province is not displayed in the tables). To check if there were differences in the factors associated with life satisfaction in rural, peri-urban, mixed, and urban areas, logistic regression models were constructed, and included main effects for the variable of interest, for the variable rurality, and for the interaction term between these two variables. Since no significant interactions were noted, the model with main effects is presented, and not separate models for categories of sociodemographic and health-related factors included in analyses. Finally, models were checked for violations of the model assumptions. All statistical analyses were conducted with SAS v9.4 (SAS, https://www.sas.com).
Ethics approval
Ethics approval for this study was granted by the University of Manitoba Bannatyne Campus Research Ethics Board (H2019:182 (HS22820)), and the study adheres to the tenets of the Declaration of Helsinki.
Results
Most adults living in rural areas had high levels of satisfaction. The baseline characteristics of the sample are shown in Table 2. Those living in rural areas were less likely to have post-secondary education, less likely to be living alone, more likely to be married, and more likely to have a lower income than those living in more urban areas. They were also more likely to be satisfied with life than those living in urban areas. The results of logistic regression models are shown in Table 3. Those living in rural areas were more satisfied with life than their urban counterparts, with those living in peri-urban and mixed regions reporting being more satisfied than those living in urban areas, but less satisfied than those living in rural areas. These associations persisted after adjusting for a wide array of health and sociodemographic factors. Also, an association was noted between a higher life satisfaction and age, as well as being female. In addition, a strong graded association was noted between income and life satisfaction. Divorced or separated individuals were less likely to have high levels of life satisfaction. Most chronic conditions were also associated with lower life satisfaction.
Table 2: Baseline characteristics of participants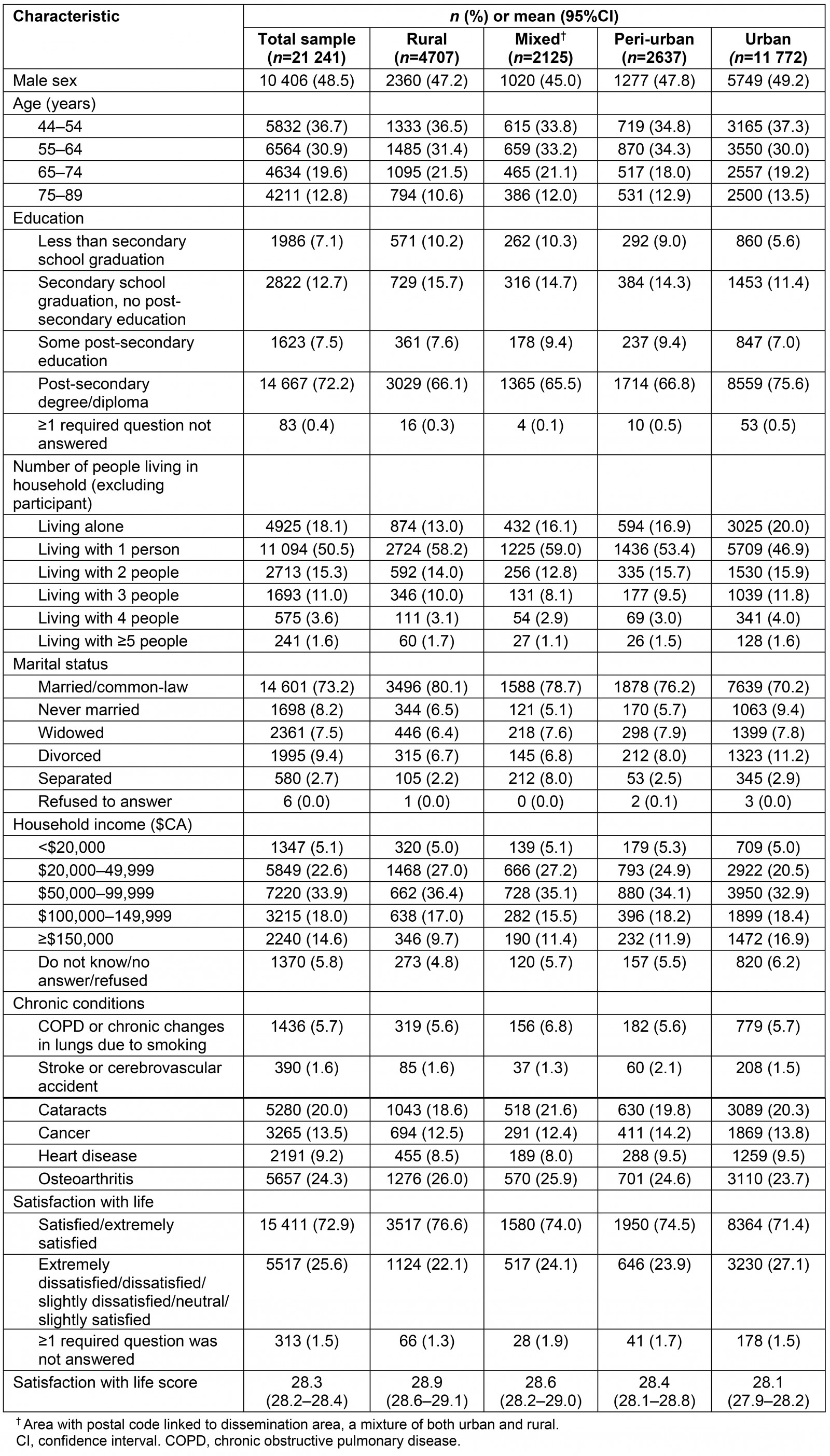
Table 3: Results of logistic regression models† for association between rural residence and satisfaction with life (satisfied/extremely satisfied)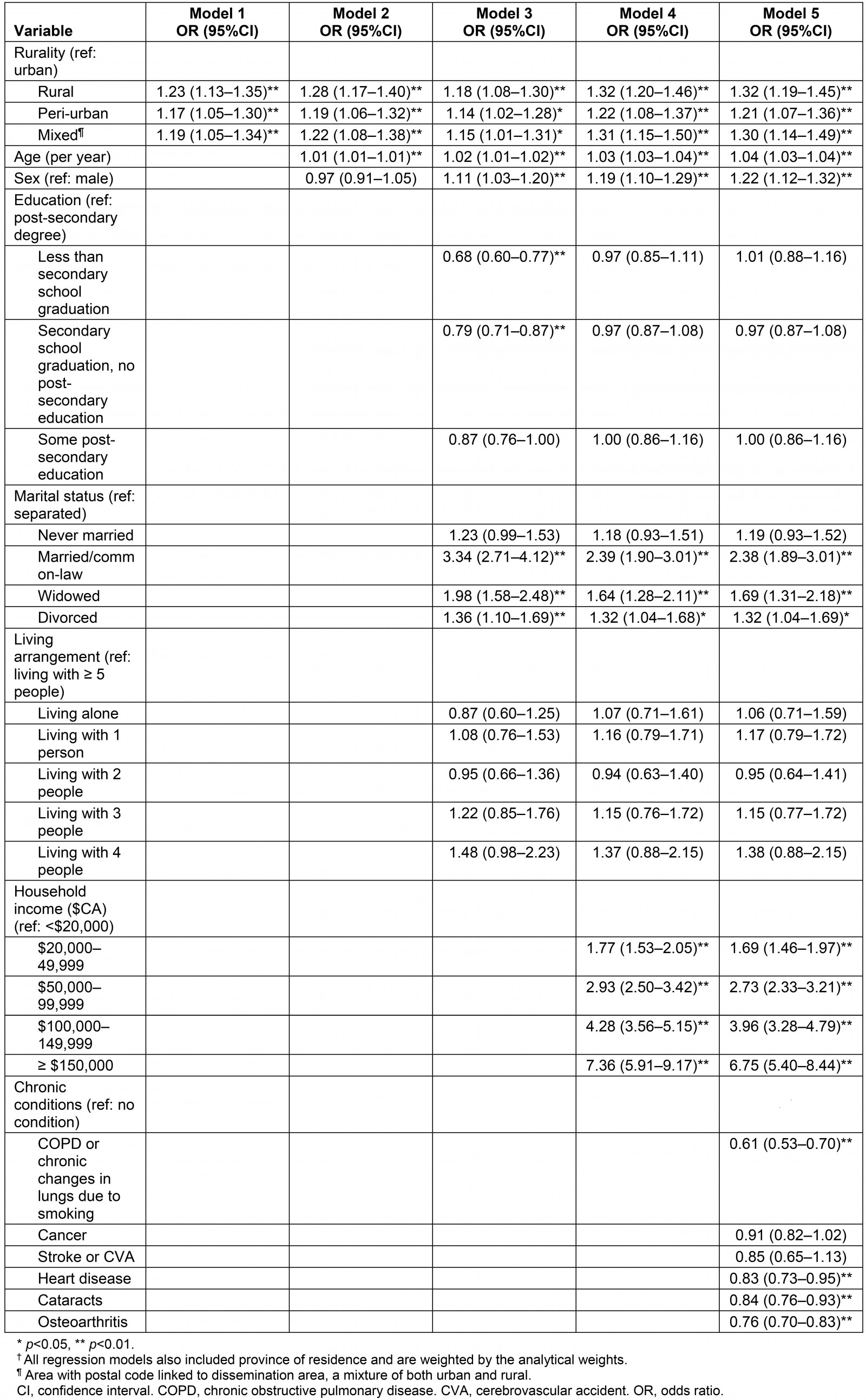
Discussion
This study examined the effect of rural residence on life satisfaction in a population-based epidemiological study and found that those living in rural areas were more likely to be satisfied with life, even after accounting for the effect of confounding factors. No interaction was found between rurality and the factors associated with life satisfaction. That is, the association of factors with life satisfaction did not differ by geographic region. However, there were factors that were associated with life satisfaction – notably that women were more likely to have higher levels of life satisfaction, that older individuals were more likely to have higher levels of life satisfaction, that those with no chronic illness were more likely to have higher levels of life satisfaction, and that those who were separated were less likely to have high levels of life satisfaction. In addition, an extremely strong association was noted between income and life satisfaction, and this appeared to be a gradient across the income categories, with no clear threshold. No association between education and life satisfaction was found. However, education was associated with other factors in the model (notably income), so this finding should be interpreted with caution.
These results are broadly similar to previous literature demonstrating that persons in rural areas appear to have higher levels of life satisfaction than their urban counterparts8,19,20. Moreover, there may be a gradient in life satisfaction, with those in urban areas being the least satisfied and those in rural regions the most satisfied, and with those in mixed and peri-urban areas having intermediate life satisfaction. Indeed, the 2020 World Happiness Report showed that happiness scores of peri-urban areas are in between the scores of rural and urban areas17, with higher scores of life satisfaction in rural areas compared to urban areas in Northern America. In contrast, on a worldwide scale, the report shows higher levels of happiness in urban areas compared to rural areas, but this difference is not apparent for highly developed countries, which is called the ‘urban paradox’17,37. The results of this study are also similar to other studies showing an association between income and/or wealth and life satisfaction, as well as health factors17-19,21. The analyses of the present study add to this by considering a representative sample, and the authors were able to account for many potential confounding factors – notably health – that some other studies could not consider.
There are both strengths and limitations in this study. A strength is that the tracking cohort of the CLSA is a population-based study intended to be as representative as possible of the Canadian population36. The first strength is that there is a large sample of rural participants in the CLSA. Second, the Satisfaction With Life Scale is a widely used measure of life satisfaction. However, it does not measure satisfaction with individual aspects of life, as some other measures do. It is possible that there are rural–urban differences in some aspects of life satisfaction (such as satisfaction with transportation) that cannot be addressed in this study. A third strength is the consideration of a gradient in rurality from large urban centers to rural areas. However, there are also weaknesses. First, there are many measures of rurality26, and this study only considered one measure. Second, as broad categories both rural and urban areas are heterogeneous38. Differences in life satisfaction between rural areas may be important, and the factors that may predict these differences could be important. Third, rural–urban differences may be dependent upon the general societal context. For instance, rural America has recently experienced economic decline, which has affected many communities in the USA, but that may not be present to the same extent in rural Canada39,40. Thus, cross-national studies should be interpreted with caution, and studies from several regions are needed. Finally, there are changes in residential setting due to moves and migration, and the effect of this on life satisfaction were not included in this study. As future waves of data collection occur, this could be addressed over time.
Conclusion
The findings of this study are important for several reasons. First, life satisfaction may be higher in rural areas than urban areas, and these differences do not appear to be due to differences in health status or income, even though differences in health status and income exist. Further research is needed into explaining the causal pathways. Second, certain interventions may prove useful to improving life satisfaction in both rural and in urban areas – notably preventing and treating common chronic illness, and also reducing inequalities in income. Finally, studies of life satisfaction should consider rurality as a potential confounding factor in analyses of life satisfaction within and across societies. The findings of this study also suggest further avenues of research. Studies that measure community-level factors may yield important insights into life satisfaction in rural areas. To date, there has been considerable interest in neighborhoods and health. Much of this has focused on urban areas, and extending these studies into rural regions may be informative. There may be elements of the natural environment, the built environment, and the nature of social connections and networks that are important in increasing life satisfaction in rural areas. Another important avenue for future research may be investigating differences between rural areas. Simply considering rural–urban differences may miss important distinctions between rural areas at regional, national, and international levels. Finally, it will be important to study changes in life satisfaction over time. Economic and social change may differentially affect life satisfaction in rural and urban areas. For instance, recent declines in economic activity appear to have affected some communities in the USA in adverse ways, and studying the effect of these social changes over time in both rural and urban settings will be important in guiding economic, social and health policy in the future.
Acknowledgements
This research was made possible using the data collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the CLSA is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference LSA 94473 and the Canada Foundation for Innovation. This research has been conducted using the CLSA dataset CLSA Baseline Tracking Dataset 3.4, under application number 19CA010. The CLSA is led by Drs Parminder Raina, Christina Wolfson and Susan Kirkland. The contents of this study were developed under a Catalyst Grant (50240) from the CIHR. We thank all participants of the CLSA.
Disclaimer: The opinions expressed in this manuscript are the author’s own and do not reflect the views of the Canadian Longitudinal Study on Aging or the CIHR.
References
You might also be interested in:
2016 - Mental health nurses in South Africa's public rural primary care settings: a human resource crisis