





Introduction
Rural medicine has long been recognised as different from urban medicine, some distinctions being broader scope of clinical practice, relative professional isolation, and essential integration in the local community. The associated perception of a less sophisticated clinical approach to patient care compared with tertiary hospital settings fails to recognise the contrast between rural and urban clinical approaches and devalues rural wisdom1. Rural doctors describe times when they push themselves to the limits of their scope of practice in order to provide the medical care required by their community. This phenomenon is called clinical courage2. This mental strength to venture out of one’s comfort zone and persevere while weighing the relative risk of alternative actions for the benefit of patients is a necessary feature of rural medicine.
Clinical courage has been described previously as including six features. First, rural doctors have a strong sense of belonging to their community, consequently choosing to stand up to serve anybody and everybody in their community. Second, rural doctors accept clinical uncertainty, recognising that they may be called on to undertake a wide range of clinical duties and, consequently, they persistently seek to prepare for clinical challenges. Third, they humbly seek to know the limits of their own clinical practice. Fourth, they work deliberately to understand and marshal resources in their context (including other clinicians and the available infrastructure) to meet the clinical demands they will face. The fifth feature relates to rural doctors needing to set aside their emotions to clear a cognitive hurdle when something needs to be done for their patient. Sixth, rural doctors described how collegial support enables rural doctors to continue to face the challenges of rural practice2.
Several of these features of clinical courage relate to rural doctors’ relationships with their community and colleagues. To further explore the role of relationships in the development of clinical courage, the authors have used Wenger’s community of practice theory as a theoretical framework. In this theory, a community of practice (rural doctors) is bound together by understandings associated with a common endeavour (providing medical care to rural patients)3. This community is sustained over time through mutual engagement (relationships), a shared repertoire (case presentations and shared stories) and communal resources the community has developed (protocols, professional development activities, ways of working)4. Communities of practice exist only when individuals come together to learn and to produce a shared praxis. Members develop an identity (as rural doctors) through participation and are drawn in from the periphery of the community (newcomer) to more engaged roles in the community (experienced members)5. Communities of practice evolve either by the development of new understandings at their core or through interactions at their boundaries4. In this article, the authors propose that clinical courage is a common lived experience for rural doctors. By using Wenger’s theory, clinical courage could be made meaningful and perpetuated through relationships within and around rural doctors’ communities of practice. After completing the initial article, the authors returned to all the interviews from the initial study and re-analysed them, looking to answer the question ‘How do interpersonal relationships impact on clinical courage?’
Methods
Participant recruitment occurred at the WONCA Rural Conference, 14th World Rural Health Conference in Cairns, Queensland, Australia. Rural doctors were invited to participate through fliers placed on seats in the conference venue. Cohort diversity was sought across a range of demographics, including gender, self-reported stage of career, and remoteness of clinical practice. Semistructured face-to-face interviews were undertaken following consent. Interviews were 30–60 minutes duration. Recordings were de-identified; they were then anonymised, transcribed, and returned to participants to review and approve prior to analysis. Further details of the methods can be found in the initial study publication2.
The authors of this article constituted a subset of the original team, all of whom are experienced rural doctors who bring their informed insider stance to this study. In this secondary analysis, the researcher team revisited all the original transcripts to consider the emic question of the impact of relationships on clinical courage. Six phases of thematic analysis were undertaken: familiarisation, coding, searching for themes, theme review, theme definition and contextualisation6. Key parts of each interview were shared with the group to identify initial codes and develop an initial coding index7. LW and RS then reviewed all the transcripts and used NVivo v12 (QSR International; https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home) to develop themes by constantly comparing transcripts, recognising patterns and finding associations until coherent descriptions emerged7. Research team members then reflected back on the original transcripts to check that participant accounts were accurately represented in the final themes.
Ethics approval
Ethics approval was granted by the Flinders University Social and Behavioural Research Ethics Committee (project number 7612).
Results
The demographics of participants from the 27 interviews is described in a previous article and consists of early career, mid-career and experienced rural doctors from Australia, Canada, New Zealand, Papua New Guinea, Scotland, South Africa and USA2. Themes that emerged from the analysis included underlying relationships with community, patient circumstances, local team relationships, discourse with other rural doctors, supporting less experienced rural doctors, facilitation of clinical courage by other medical colleagues, and challenges to rural doctors’ ways of working.
Underlying relationships with community create the foundation for clinical courage
The responsibility to provide medical care for a community was described as grounded in relationships with community members, valuing their world view, and seeking to reciprocate.
I think in our nature we constantly have a strong appreciation of the community’s world view on health. (25)
The other times when I've felt that I was outside my comfort zone was when I've had patients insist that I manage their care, when I would usually hand over to a specialist. (9)
Rural communities were often very appreciative of rural doctors.
I think that sense of altruism and knowing how what we do will positively impact on the communities or our patients as a whole, that’s something that is a really powerful tool for us because we can feed off the gratitude, you can feed off the fact that you are making differences in rural communities. (20)
This sense of privileged belonging in the community could extend beyond the doctor to spouses and other family members. Collective community trust in the doctor develops over time, and enables doctors to feel trusted to broaden their scope of practice, trusting the community members will support them in return. This was particularly important in more remote locations.
We live in the hospital, the house is in the hospital so it’s all the time, there’s no hours … in reality night times I’m usually working, weekends I’m usually working as well. I think that’s actually pretty common in very remote medical practice, the distinction between work and life gets a lot more blurry … The community is surrounding me, they’re looking after me and so it’s okay, I can do the things that I think I’m competent to do. (22)
This close integration with the community could create messy personal boundaries. Occasionally, these blended relationships could cause significant distress; for example, one doctor talked about when another member of the clinical team was gravely ill.
I think definitely, in the moment, you don’t think it’s traumatising for you, but definitely having a friend, who is also a colleague, but then became quickly a patient, was incredibly distressing. I think in other settings you would morally and ethically probably not treat her; it wouldn’t be your responsibility, because you would have people around you that you could share … the management with and you would never be asked to treat those people. (25)
On other occasions the relationships with community caused more insidious risks to doctors.
With competence, comes more and more responsibilities, more and more ownership of the community and integration into the community. And that’s not always a sustainable approach. (25)
Patient circumstances influence clinical decisions
All participants frequently described drawing on clinical courage to manage patients with time-dependent emergency presentations, particularly when required to undertake unfamiliar or more complex clinical procedures. Importantly, participants also described non-acute patient presentations, when patients were unable or unwilling to travel away from their community to access care, which created circumstances where the doctor felt a responsibility to provide medical care. Examples given included oncology follow-up after initial chemotherapy, and managing chronic renal disease, complex dermatological conditions and complex mental illness. Part of managing these patient relationships involved explicit discussions and exploration with the patient about expectations of care, management alternatives and their risks, and the level of risk an individual patient was prepared to take on.
I had had a good discussion with the patient about where the limits of my practice would usually be, and that I would usually ask for some assistance from a specialist colleague. But they insisted that this was how they wanted their care managed, and you feel that it's better that the patient is engaged, rather than not engaged with any health professionals. (9)
Letting them be aware [of the risks]. If they feel uncomfortable about that, then that will affect my decision making. You can assume a lot about what risk that other people are prepared to take, but I think you’re much better to have an open discussion about it. (11)
Local team relationships underpin clinical courage
In the interviews, there was frequent reference to working as part of a team and the value of having other experienced clinicians (doctors and nurses) around when called on to manage a case outside one’s usual experience, because these people offered clinical expertise, moral support or just safety in numbers.
I had a skilled emergency nurse with me who was really good support. And we had enough equipment just to do an intubation. (12)
So the first thing that happened was that because we have a lot of really good collaborative team players, was that suddenly everybody started appearing in that emergency department. So, one of the docs who's very good at emergency procedures showed up, and two nurses came in who are the experienced nurses, and suddenly there was a whole team of us, and then that was before the guy [trauma case] even got there. And then the guy comes in and everything's like it's a whole different ball game, when you have four or five or six of you to work on somebody, than if you just have yourself. (21)
Skill mix was considered not only in terms of senior medical staff but also in terms of nursing and paramedical team members. Sometimes, the human resources were ad hoc, such as visitors to town.
I had trainees who were there with me, two of whom had just done their neonatal intensive care rotation at the university so they were there to help the two paediatricians who happened to be in town that weekend, stabilised the two infants while I and another resident delivered the babies. Our obstetrician came in from home and he ran the ultrasound as we delivered the twins, to monitor the second twin and also to be there should we have to go to caesarean for the benefit of the second twin. And so it was in that moment that I was struck with how excellent the care was, not because any one of our individual expertise but because of our collective expertise and our relationships. I had practised with this obstetrician for more than a decade so we knew each other’s skills, he trusted me I trusted him; the nurses pitched in. Yep that woman got outstanding care. But it was at the limits of my competence. (1)
Cohesive and functional teams enabled doctors to undertake procedures at the edge of their scope. However, clinical courage was also needed at times when there were differences in opinions between local team members.
Probably where you need most courage is to say, ‘This patient doesn't need to be moved at this stage’. So when the nurses are going, ‘No, no, we’re not used to looking after patients like this’ to actually say, ‘This is not in the patient’s best interests to move them. It’s a stable patient, we’ve got the skills, they want to be close to their family, it’s going to cost us a whole heap of money, none of those things need to happen, let’s keep them’. That takes some courage and the system from on high doesn't always lend itself to that. (22)
Discourse with other rural doctors
Trusted colleagues enabled self-reflection. Rural doctors described relying on their own network of like-minded colleagues to get timely advice to support patient care, to debrief, to benchmark and to learn new skills. Participants reported that this network did not have to be co-located. Here is an example of an online network built around a rural physician listserv.
So say through the Society of Rural Physicians of Canada, I’m pretty involved with them … Some of the courses that they’ve offered are opportunities for you to debrief and reinforce for yourself and validate for yourself some of these things that you need to do. It’s a source of ideas when you’re in some of these situations, but also a source of support … People will post about a situation that they had and then all of a sudden you see five other people that are writing … So it helps to bridge some of those gaps. (18)
Close colleagues of many years were seen as a good sounding board and helped rural doctors to maintain clinical courage. Colleagues were especially important when rural doctors had acted at the edge of their comfort zone and patients had poor outcomes.
… to discuss and debrief and reflect and not hold it in. Because I think we are always our own worst critics in terms of a situation like that [poor patient outcome]. So it’s nice to have a general sense of how things went and get feedback. I have a really close colleague I’ve been practising with for 25 years and so he’s a really a good sounding board. We’re always asking each other clinical questions. We discuss difficult cases too. So I think that’s been very helpful. (23)
Supporting less experienced rural doctors
Participants described examples of being supported by senior colleagues. Others described deliberately supporting less experienced rural doctors with specific procedures.
The chest tube was difficult because he had so much surgical emphysema, and he was a big guy anyway … When it came to the intubation, what actually happened was that I ended up doing it because [junior colleague] had got herself into a bit of a fluster. And I could see that we were running out of time, as far as the drugs were concerned for intubation, and I took over … We have had a good discussion about that, since, because I felt, afterwards, ‘Did I do the right thing, taking over?’ As far as the patient was concerned, probably yes, but … for [junior colleague]’s confidence – that's one of the things we had to talk about. About how we might get set up next time, to try and improve her chances of success. (9)
One participant described how relationships with colleagues resulted in significant expectation and pressure to push the boundaries when commencing a new role.
I started in my rural practice [many years ago] … the seniors for the practice called me, and said they had an appendectomy and could I come and do the anaesthetic … And I said to them, ‘I have no problem coming to help you’ … ‘I haven’t done anaesthesia for two years, I’m happy to assist or whatever.’ But they said, ‘No, no you have the papers, you come and do the anaesthetic’. And I just had to walk in there in a brand new operating room, brand new anaesthetic machine, and sort things out. It was a little kiddie of twelve years old and I was scared shitless, but in the end it worked fine. So sometimes people push you into the situation. (7)
Within a supported rural environment, clinical courage developed over time.
What I saw with the residents who came to our program was that many of them came without a strong sense of that [clinical courage], but by seeing it modelled by those of us who were already there and then by having the opportunity to venture and succeed built courage over time. So to me it's all about the opportunity to risk and succeed. It's safe because you're doing it with others and you're doing it with others who are more senior. (1)
Facilitation of clinical courage by other medical colleagues
Other medical colleagues familiar with, and respectful of, the context of rural practice could facilitate rural doctors’ clinical courage.
I spoke to a specialist anaesthetist who is based in [community], which is another remote area, and he was really useful because he basically called the situation as it was. He said, ‘Look, you’re probably going to kill him. This is really hard. These are the drugs I’d use. You’ve got to give it your best shot’. And that was a really steadying influence. If I hadn’t had him, I think I really would have struggled, because … [he] just brought back my focus to what I had to do. (12)
Even from a distance, timely discourse with trusted colleagues supported doctors in exploring the risks and benefits of proposed management plans. One island doctor described being involved in rescuing a young man from a car partway down a cliff in a storm, and then managing his head injury in a small rural hospital with little support because the storm was too ferocious for a retrieval. He felt comfortable managing the acute injury, but he needed clinical courage later, when the young man returned following months of rehabilitation on the mainland. At this point, he assessed the risk of personally providing cognitive behavioural therapy, a technique he was not previously familiar with.
The system didn't support going outside the box [to deliver cognitive behavioural therapy locally], hence why it required the courage. It would have been nice to say to someone ‘look, I'd like to do this, would this be the right thing?’ I used my friend actually who was a senior [psychiatry] trainee at that point. So I obviously trusted that advice professionally as well as knowing her as a friend. (13)
In recent years, telehealth systems have made it easier to share responsibility for decisions and to be supported to learn.
I've got a patient just recently diagnosed with thyrotoxicosis … She’s had a recent shoulder replacement, she’s got a bad knee, she's recently been diagnosed with Parkinson's disease … For her to travel to see an endocrinologist would be quite challenging … Being able to access that service, through telehealth, has made her life much easier, and given me a little bit of hand-holding from the specialist colleague. (9)
Challenges to rural doctors’ ways of working
Rural doctors described working differently from, perhaps more innovatively than, their city peers. Criticism from specialists or other sources could constrain rural doctors’ clinical courage.
I think rural doctors, we’re always challenging norms, we’re always looking for innovations, better ways to improve patient care, and there are always going to be people that are resistant to that. Maybe not in the sense that you have significant workplace problems, but to the sense where people may discredit some of the work that you do. (20)
Discordant relationships with health system hierarchy were seen as another threat to the way rural doctors work, particularly when outsiders were seen to have the power to enable or prevent doctors from undertaking clinical activities.
… limiting scope of practice and specialists saying ‘well you shouldn’t do that as a GP’. We’re actually limiting what people do and at the end of the day it’s the patients that suffers. (10)
If then you have to fight that battle as well as your own internal battle, to say ‘do I think I can do this?’ Then it's too easy to give up. (27)
On the other hand, medical colleagues with a poor understanding of the clinical context could jeopardise rural practice by expecting too much of rural doctors. One participant recalled a story about a baby with bronchiolitis who she was trying to transfer. The initial response from the paediatrician in the city was that they could do little more for the patient and were loath to accept a patient transfer from the rural hospital. This clinical decision did not recognise how stretched the rural hospital staff were, or the risk of transporting the baby should he deteriorate.
You [the rural physician] have the right to say no [to the urban specialist] if it just feels wrong to you or too dangerous to you or the patient. Some stuff is cowboy stuff and you shouldn’t be doing it. (7)
Discussion
This study found that clinical courage was impacted on by the relationships rural doctors had with their communities and patients, with each other, with the local members of their healthcare team and with other colleagues and health leaders outside their immediate community of practice (Fig1). These groups act at what Wenger calls the ‘nexus of multiple membership’8.
Lave and Wenger describe a community of practice as a formal or informal group that engages in learning to perpetuate a way of being that they value within a specific discipline or field3. This study positions rural doctors as sharing a community of practice committed to the enterprise of providing medical care to the community of rural people they choose to serve.
Individual relationships with a rural community can be understood as social capital that has two distinct components: trust and association9. Trust relates to reliable symbiotic engagement, whereas association refers to the neighbourly behaviours that produce familiarity, such as informal socialising or assistance to complete a day-to-day task10. Social capital is embedded within the individual (rural doctor) and the group (local community)9. This relationship with and commitment to rural people has been previously demonstrated as a common purpose shared by members of the community of practice. The authors refer to this feature as ‘standing up to serve anybody and everybody in the community’2; they argue that this sets rural doctors apart from other similar medical communities of practice where there is a general desire to serve people well, without this being socially or geographically bound to a collective of people11.
These findings suggest that rural doctors’ community of practice facilitates clinical courage to be conceived and judged by members as a meaningful characteristic of their way of working8. Members of the community of practice described valuing clinical courage as a means to broaden their scope of practice while pragmatically managing the risks to patients associated with infrequent use of some clinical skills. Relationships between members enable individuals to adopt the culture and language used by the community of practice regarding clinical courage to share stories of clinical encounters for the purposes of debriefing, benchmarking with trusted peers, maintaining expertise and learning additional skills from each other. Bandura, in his social cognition theory of self-efficacy (1997), suggests the possibility of ‘vicarious mastery’12. When people see or hear of how other people similar to themselves successfully performed a task, this extends their beliefs in their own potential abilities. Perhaps more importantly, within the context of a community of practice, clinical courage can be considered a collective efficacy, which is defined as ‘a group's shared belief in its conjoint capability to organise and execute the courses of action required to produce given levels of attainment’12.
Rural doctors described their relationships with less experienced members of the community of practice, which focused on engaging them to observe, seek out and adopt similar responsibility for a rural community, clinical epistemology, and scope of practice. The community of practice members sought to perpetuate clinical courage by intentionally encouraging trainees to use their skills, stepping back to enable them to undertake procedures and engaging when necessary to maintain patient safety, then debriefing to prepare trainees better for the next clinical courage occasion. Facilitating legitimate participation in rural patient care is consistent with Wenger’s description of how ‘newcomers’ are embraced by and enter into membership of a community of practice4. Members are constantly evolving the norms of the community of practice and while clinical courage was highly valued in this study, there were alternative (less prominent) discourses seeking to push back when communities expect too much from their rural doctors, risking unsafe patient care or unsustainable work conditions for individual doctors. The authors hope this article will precipitate further discourse among rural doctors regarding clinical courage and its place in the community of practice.
The context of rural medicine challenges rural doctors and their local health team members to value place (including cultural meaning of travel, dislocation and returning home for individual rural patients); and to value community (how patients understand themselves, solidarity, reciprocity and not wanting to be a burden)13.
Relationships with local health personnel and knowledge of the resources available in their community enabled participants to tap into the skills of the team, a feature the authors describe as ‘deliberately understanding and marshalling resources in the context’. The rural doctor community of practice valued local clinical teams highly, with stories recognising the collective contribution of other doctors, nursing staff and paramedics within the rural health service. These relationships, while still bound by the traditional medical culture of clinical hierarchy, suggest clinical courage is practised where healthcare teams know and trust the skills of each member as more equal partners in the enterprise of rural medical care. The evidence demonstrates that these relationships take time to develop. This has significant implications for medical care in the context of rural hospitals dominated by locums or doctors undertaking compulsory community/government service, where transient doctors will not have established relationships with other team members.
Bridging social capital is what Paxton (1999) refers to as cross-cutting ties10. Bridging social capital occurs when members of one group connect with members of other groups to seek access or support or to gain information. Relationships with doctors who know and respect the rural clinical context as well as with colleagues who demonstrate trust in and respect for an individual rural doctor enabled rural doctors to practise clinical courage, by providing ‘collegial support to stand up again’. Learning was facilitated when rural doctors obtained sympathetic opinions about specific patient conditions and the clinical challenges they faced. As well as supporting individual doctors, these sympathetic colleagues can strengthen external recognition of clinical courage as a way of being for rural doctor members of the community of practice.
Other doctors and health leaders outside the community of practice, not committed to the enterprise of rural medical practice, can undermine rural doctors’ clinical courage, when they pass judgement or place obstacles in the way of rural doctors seeking to care for their patients. The unique element of the rural doctor community of practice is the innate relationship with the community. It is this relationship that is at the core of rural doctors’ experience of clinical courage. This is perhaps poorly understood by urban colleagues, whose experience of their own community of practice does not include such a strong commitment to and immersion in a distinct population. Clinical discomfort tends to trigger clinicians, particularly less experienced clinicians, to lean on others to manage uncertain situations14. Limit setting and critique by outsiders may indicate less experience with rural health care, or an attitude of geographical narcissism1, or an appropriate concern for quality and safety. Whichever it may be, these sentiments provide an opportunity for individual doctors and importantly the community of practice to engage in critical self-reflection. This can lead to an integration of new knowledge into the praxis of rural medicine, or challenge restrictions placed on the community of practice.
With the rapid pace of change in medicine, the nexus between the community of practice of rural medicine and medicine more generally provides an opportunity for ongoing discourse to define and refine clinical courage as a way of being for rural doctors.
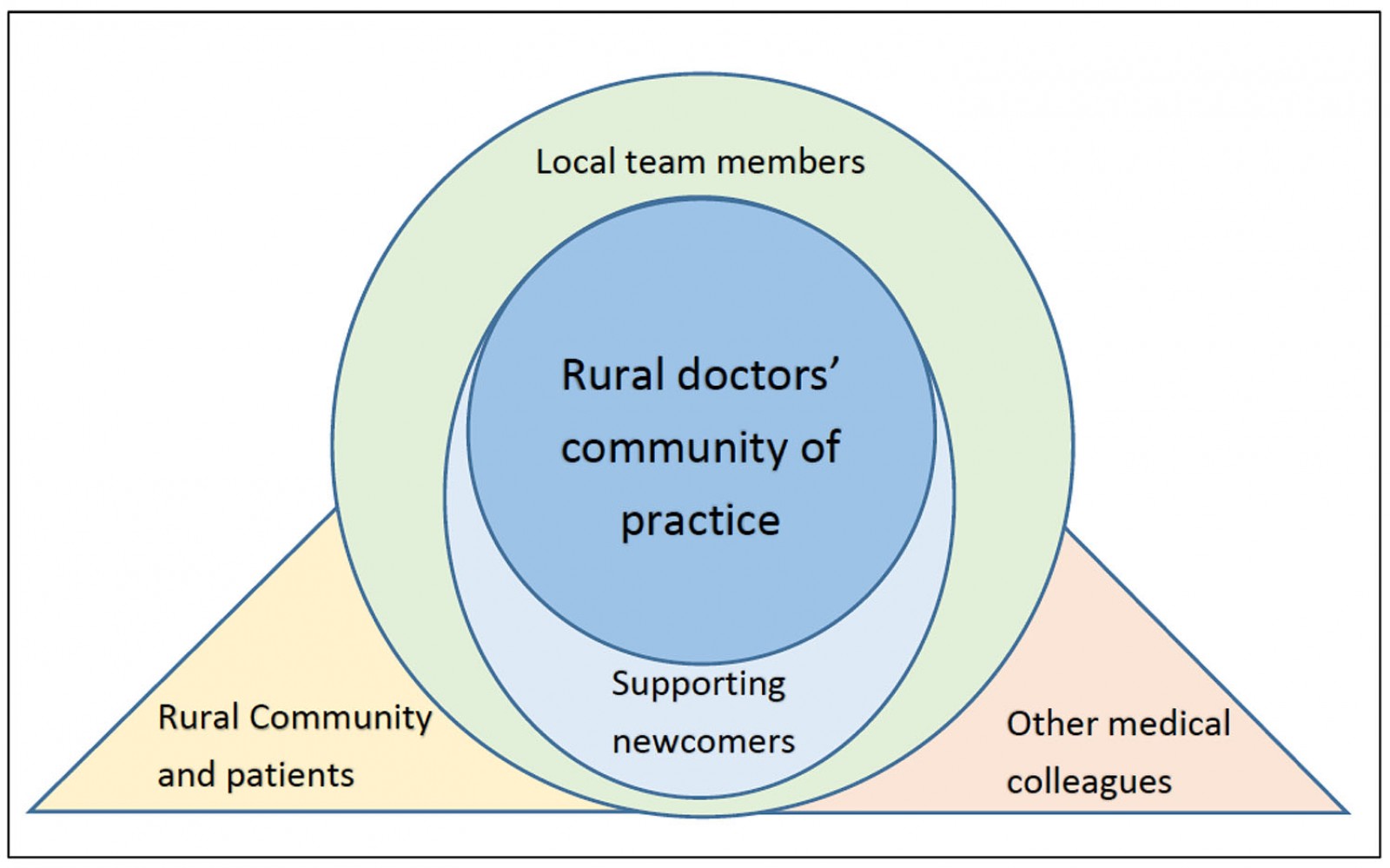 Figure 1: Rural doctors’ community of practice and relationships with other significant groups that influence clinical courage.
Figure 1: Rural doctors’ community of practice and relationships with other significant groups that influence clinical courage.
Conclusion
Using communities of practice as a conceptual framework, this study demonstrates that rural doctors collectively learn and use clinical courage based on the relationships that are central to practice in the rural context. Relationships with rural communities, rural patients and urban colleagues can foster the clinical courage of rural doctors. Importantly, experienced rural doctors can support the development of clinical courage in new members of the discipline. While the discourse of detractors can challenge clinical courage, this discourse at the boundaries of the community of practice requires individual rural doctors and their community of practice to champion clinical courage and be intentional about rural doctors’ way of working.
Acknowledgements
Thanks to Dr Ella Cockburn and Dr Laura Grave for undertaking the interviews for this study while they were medical students. Thanks to Dr Susan Williams, for her careful critique and gentle feedback on manuscript drafts.
References
You might also be interested in:
2021 - Grey nomads with diabetes self-management on the road – a scoping review
2006 - Increased prevalence of diabetes mellitus in a rural Greek population